Cathy J Bradley, Rifei Liang, Richard C Lindrooth, Lindsay M Sabik, Marcelo C Perraillon
{"title":"High-Cost Cancer Drug Use in Medicare Advantage and Traditional Medicare.","authors":"Cathy J Bradley, Rifei Liang, Richard C Lindrooth, Lindsay M Sabik, Marcelo C Perraillon","doi":"10.1001/jamahealthforum.2024.4868","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>Medicare Advantage (MA) plans are designed to incentivize the use of less expensive drugs through capitated payments, formulary control, and preauthorizations for certain drugs. These conditions may reduce spending on high-cost therapies for conditions such as cancer, a condition that is among the most expensive to treat.</p><p><strong>Objective: </strong>To determine whether patients insured by MA plans receive less high-cost drugs than those insured by traditional Medicare (TM).</p><p><strong>Design, setting, and participants: </strong>This cohort study used data from the linked Colorado All Payer Claims Database and Colorado Central Cancer Registry. This population-based cohort included adults 65 years and older insured by Medicare with prescription coverage who reside in Colorado and were diagnosed with colorectal (CRC) or non-small cell lung cancer (NSCLC) between January 2012 and December 2021. The data were analyzed between December 2023 and August 2024.</p><p><strong>Exposure: </strong>Enrollment in TM or MA insurance plans.</p><p><strong>Main outcomes and measures: </strong>Claims for chemotherapy and oral targeted agents were identified. Thresholds for high-cost drugs were based on the distribution of drug costs. Inverse probability weighted logistic regression for receiving any cancer drug and for receiving a high-cost cancer drug was estimated, controlling for patient and ecological characteristics. The sample was stratified by cancer site and local/regional and distant stage.</p><p><strong>Results: </strong>Of 4240 patients included in the analysis (mean [SD] age, 75 [7] years; 2327 [54.9%] female), 1991 were diagnosed with CRC and 2249 with NSCLC. A total of 1647 patients had local or regional CRC, and 344 had distant CRC; 1351 patients had local or regional NSCLC, and 898 had distant NSCLC. In the covariate-adjusted analysis, patients diagnosed with local or regional CRC who were insured by MA were 6.0 percentage points less likely to receive a cancer drug than similar patients insured by TM. Patients diagnosed with distant NSCLC were 10.0 percentage points less likely to receive a cancer drug if insured by MA. Among patients who received a cancer drug, patients insured by MA were less likely to receive a high-cost drug for local or regional CRC (by 10.0 percentage points) and distant CRC (by 9.0 percentage points).</p><p><strong>Conclusions and relevance: </strong>In this cohort study, high-cost drugs were more commonly prescribed among patients enrolled in TM and diagnosed with CRC. A similar pattern was not observed for patients with NSCLC, perhaps because clinical evidence suggests survival benefits to be associated only with certain drugs, all of which are expensive. Nonetheless, MA was modestly associated with reduced high-cost drug utilization and may reduce overall treatment costs.</p>","PeriodicalId":53180,"journal":{"name":"JAMA Health Forum","volume":"6 1","pages":"e244868"},"PeriodicalIF":11.3000,"publicationDate":"2025-01-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11724345/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JAMA Health Forum","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1001/jamahealthforum.2024.4868","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: Medicare Advantage (MA) plans are designed to incentivize the use of less expensive drugs through capitated payments, formulary control, and preauthorizations for certain drugs. These conditions may reduce spending on high-cost therapies for conditions such as cancer, a condition that is among the most expensive to treat.
Objective: To determine whether patients insured by MA plans receive less high-cost drugs than those insured by traditional Medicare (TM).
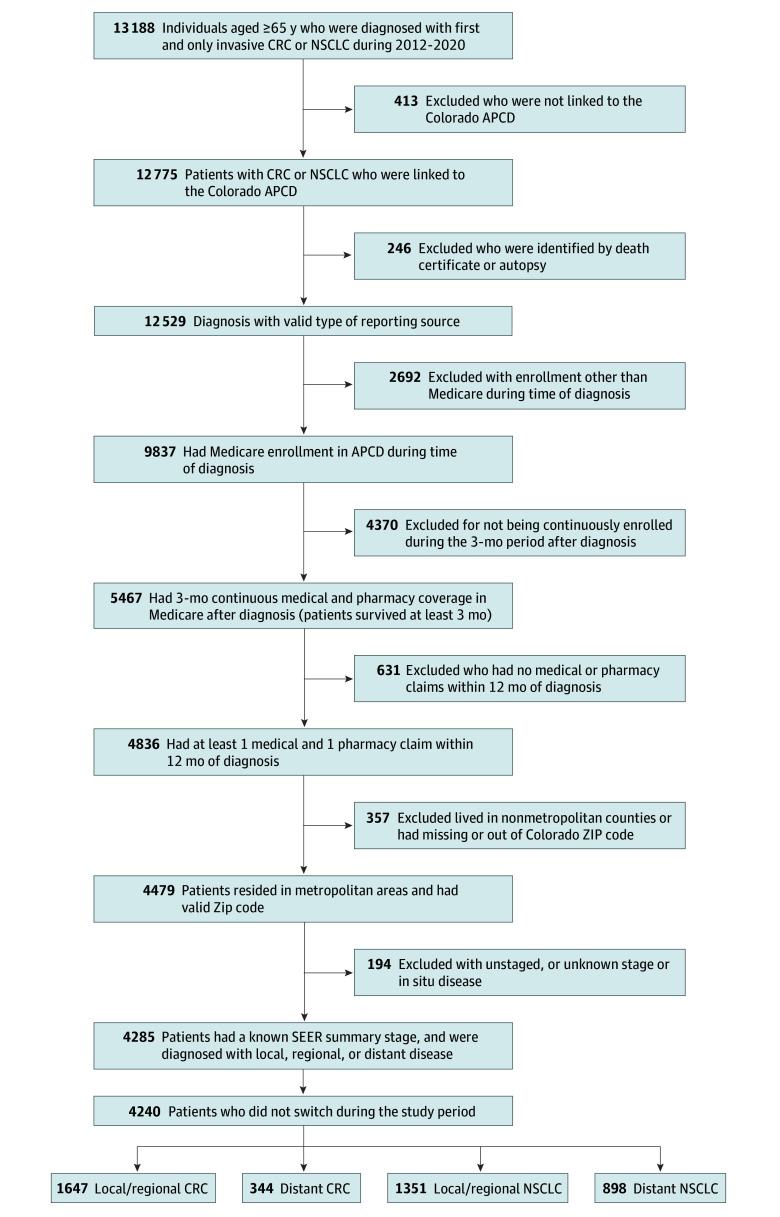
Design, setting, and participants: This cohort study used data from the linked Colorado All Payer Claims Database and Colorado Central Cancer Registry. This population-based cohort included adults 65 years and older insured by Medicare with prescription coverage who reside in Colorado and were diagnosed with colorectal (CRC) or non-small cell lung cancer (NSCLC) between January 2012 and December 2021. The data were analyzed between December 2023 and August 2024.
Exposure: Enrollment in TM or MA insurance plans.
Main outcomes and measures: Claims for chemotherapy and oral targeted agents were identified. Thresholds for high-cost drugs were based on the distribution of drug costs. Inverse probability weighted logistic regression for receiving any cancer drug and for receiving a high-cost cancer drug was estimated, controlling for patient and ecological characteristics. The sample was stratified by cancer site and local/regional and distant stage.
Results: Of 4240 patients included in the analysis (mean [SD] age, 75 [7] years; 2327 [54.9%] female), 1991 were diagnosed with CRC and 2249 with NSCLC. A total of 1647 patients had local or regional CRC, and 344 had distant CRC; 1351 patients had local or regional NSCLC, and 898 had distant NSCLC. In the covariate-adjusted analysis, patients diagnosed with local or regional CRC who were insured by MA were 6.0 percentage points less likely to receive a cancer drug than similar patients insured by TM. Patients diagnosed with distant NSCLC were 10.0 percentage points less likely to receive a cancer drug if insured by MA. Among patients who received a cancer drug, patients insured by MA were less likely to receive a high-cost drug for local or regional CRC (by 10.0 percentage points) and distant CRC (by 9.0 percentage points).
Conclusions and relevance: In this cohort study, high-cost drugs were more commonly prescribed among patients enrolled in TM and diagnosed with CRC. A similar pattern was not observed for patients with NSCLC, perhaps because clinical evidence suggests survival benefits to be associated only with certain drugs, all of which are expensive. Nonetheless, MA was modestly associated with reduced high-cost drug utilization and may reduce overall treatment costs.
期刊介绍:
JAMA Health Forum is an international, peer-reviewed, online, open access journal that addresses health policy and strategies affecting medicine, health, and health care. The journal publishes original research, evidence-based reports, and opinion about national and global health policy. It covers innovative approaches to health care delivery and health care economics, access, quality, safety, equity, and reform.
In addition to publishing articles, JAMA Health Forum also features commentary from health policy leaders on the JAMA Forum. It covers news briefs on major reports released by government agencies, foundations, health policy think tanks, and other policy-focused organizations.
JAMA Health Forum is a member of the JAMA Network, which is a consortium of peer-reviewed, general medical and specialty publications. The journal presents curated health policy content from across the JAMA Network, including journals such as JAMA and JAMA Internal Medicine.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
