Mohamed Shanshal, Joseph Maakaron, Kaushal Parikh, Jenesse Nicole Moffett, Ailsa G Luce, Anna J Schwecke, Julian Molina, Konstantinos Leventakos
{"title":"Unusual outcome of treatment of thymoma with immunotherapy: case report.","authors":"Mohamed Shanshal, Joseph Maakaron, Kaushal Parikh, Jenesse Nicole Moffett, Ailsa G Luce, Anna J Schwecke, Julian Molina, Konstantinos Leventakos","doi":"10.21037/med-24-20","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Thymoma is a rare mediastinal neoplasm originating from thymic epithelial cells, often associated with paraneoplastic syndromes. These syndromes can manifest as a range of autoimmune disorders, including myasthenia gravis, pure red cell aplasia, and aplastic anemia. Clinical trials involving the use of immune checkpoint inhibitors (ICIs) in thymoma have been complicated by a high incidence of immune-related adverse effects (irAEs). As a result, the use of ICIs in the treatment of thymoma is not currently recommended.</p><p><strong>Case description: </strong>We present a case of thymoma with paraneoplastic aplastic anemia that showed a remarkable response to atezolizumab following the discontinuation of cyclosporine. The patient was initially treated with cisplatin, doxorubicin, and cyclophosphamide (CAP), achieving a short-term partial response. However, this response was not sustained, and she developed aplastic anemia characterized by worsening anemia, reticulocytopenia, and thrombocytopenia. A bone marrow biopsy revealed erythroid hypoplasia without dysplasia, linked to her thymoma. Cyclosporine was initiated to manage the aplastic anemia, but the disease continued to progress, leading to a switch to capecitabine and gemcitabine. Restaging scans revealed further advancement, with extensive pleural metastasis. To manage the progressing disease, atezolizumab was introduced. Initially, no response was seen while on cyclosporine, but after discontinuing cyclosporine, the patient experienced a significant therapeutic response. Despite this success, immune-related dermatitis and hematological complications developed, requiring careful management. In clinical trials, ICI use alongside immunosuppressants is common for managing paraneoplastic manifestations in thymoma.</p><p><strong>Conclusions: </strong>This case highlights the potential efficacy of ICI in thymoma treatment, emphasizing the delicate balance required between immunosuppression and immunotherapy for optimal outcomes. Achieving this delicate balance is vital for optimizing patient outcomes while minimizing the risk of severe complications and ensuring that both the paraneoplastic syndrome and the tumor itself are adequately managed. This consideration is particularly important when developing future clinical trials for thymoma, where the complex interplay between these therapies must be carefully evaluated to design effective and safe treatment protocols.</p>","PeriodicalId":74139,"journal":{"name":"Mediastinum (Hong Kong, China)","volume":"8 ","pages":"54"},"PeriodicalIF":0.0000,"publicationDate":"2024-11-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11707440/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Mediastinum (Hong Kong, China)","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.21037/med-24-20","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Thymoma is a rare mediastinal neoplasm originating from thymic epithelial cells, often associated with paraneoplastic syndromes. These syndromes can manifest as a range of autoimmune disorders, including myasthenia gravis, pure red cell aplasia, and aplastic anemia. Clinical trials involving the use of immune checkpoint inhibitors (ICIs) in thymoma have been complicated by a high incidence of immune-related adverse effects (irAEs). As a result, the use of ICIs in the treatment of thymoma is not currently recommended.
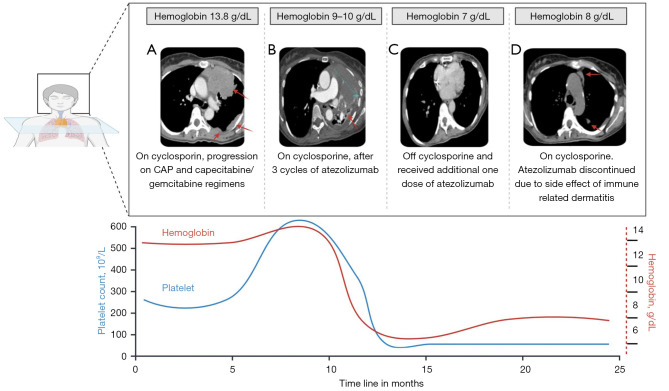
Case description: We present a case of thymoma with paraneoplastic aplastic anemia that showed a remarkable response to atezolizumab following the discontinuation of cyclosporine. The patient was initially treated with cisplatin, doxorubicin, and cyclophosphamide (CAP), achieving a short-term partial response. However, this response was not sustained, and she developed aplastic anemia characterized by worsening anemia, reticulocytopenia, and thrombocytopenia. A bone marrow biopsy revealed erythroid hypoplasia without dysplasia, linked to her thymoma. Cyclosporine was initiated to manage the aplastic anemia, but the disease continued to progress, leading to a switch to capecitabine and gemcitabine. Restaging scans revealed further advancement, with extensive pleural metastasis. To manage the progressing disease, atezolizumab was introduced. Initially, no response was seen while on cyclosporine, but after discontinuing cyclosporine, the patient experienced a significant therapeutic response. Despite this success, immune-related dermatitis and hematological complications developed, requiring careful management. In clinical trials, ICI use alongside immunosuppressants is common for managing paraneoplastic manifestations in thymoma.
Conclusions: This case highlights the potential efficacy of ICI in thymoma treatment, emphasizing the delicate balance required between immunosuppression and immunotherapy for optimal outcomes. Achieving this delicate balance is vital for optimizing patient outcomes while minimizing the risk of severe complications and ensuring that both the paraneoplastic syndrome and the tumor itself are adequately managed. This consideration is particularly important when developing future clinical trials for thymoma, where the complex interplay between these therapies must be carefully evaluated to design effective and safe treatment protocols.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
