{"title":"Approaches for difficult-to-induce-seizures electroconvulsive therapy cases (DEC): a Japanese expert consensus.","authors":"Yoshiteru Takekita, Taro Suwa, Kazuyuki Yasuda, Hirotsugu Kawashima, Wataru Omori, Naoki Kurimoto, Takashi Tsuboi, Takamasa Noda, Nobuatsu Aoki, Ken Wada, Ken Inada, Minoru Takebayash","doi":"10.1186/s12991-024-00543-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Seizure threshold increases with age and the frequency of electroconvulsive therapy (ECT). Therefore, therapeutic seizures can be difficult to induce, even at maximum stimulus charge with available ECT devices. Such cases are known as difficult-to-induce-seizures electroconvulsive therapy cases (DECs). However, no clinical guidelines exist for DECs; thus, clinicians often face difficulties determining treatment strategies. This study aimed to obtain a consensus among clinical experts regarding the treatment of DECs.</p><p><strong>Methods: </strong>We asked Japanese ECT experts to rate 14 approaches under six conditions of DECs on a 9-point Likert scale (1 = \"disagree\" to 9 = \"agree\"). Based on responses from 195 experts, the approaches were classified as first-line (95% confidence interval mean ≥ 6.5), second-line (mean, 3.5-6.5), or third-line strategies (mean < 3.5). Approaches rated 9 points by at least 50% of the respondents were considered \"treatments of choice.\"</p><p><strong>Results: </strong>To avoid difficult seizure induction, dose reduction of benzodiazepine receptor agonist (BZRA) (8.33 ± 1.25), dose reduction or discontinuation of antiepileptic drugs (AEDs) or other drugs that may make seizure induction difficult (8.16 ± 1.18), and ensure hyperventilation (7.95 ± 1.47) were classified as treatments of choice. First-line treatment strategies were BRZA discontinuation (7.89 ± 1.45), stimulation timing adjustment (7.00 ± 2.00), and anesthetic dose reduction (6.93 ± 1.94). Dose reduction or discontinuation of AEDs or other drugs that might make seizure induction difficult and ensure hyperventilation were the treatments of choice across all patient conditions. The results of rating approaches for patients with mood disorders and schizophrenia were similar, with differences observed among the approaches for patients with catatonia, high risk of cognitive impairment, and cardiovascular events.</p><p><strong>Conclusions: </strong>ECT expert recommendations are useful and can assist in clinical decision-making. Our results suggest that while some strategies are applicable across all conditions, others should be tailored to meet the specific needs of patients. These recommendations should be further evaluated in future clinical studies.</p>","PeriodicalId":7942,"journal":{"name":"Annals of General Psychiatry","volume":"24 1","pages":"2"},"PeriodicalIF":3.6000,"publicationDate":"2025-01-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11727425/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of General Psychiatry","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12991-024-00543-9","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Seizure threshold increases with age and the frequency of electroconvulsive therapy (ECT). Therefore, therapeutic seizures can be difficult to induce, even at maximum stimulus charge with available ECT devices. Such cases are known as difficult-to-induce-seizures electroconvulsive therapy cases (DECs). However, no clinical guidelines exist for DECs; thus, clinicians often face difficulties determining treatment strategies. This study aimed to obtain a consensus among clinical experts regarding the treatment of DECs.
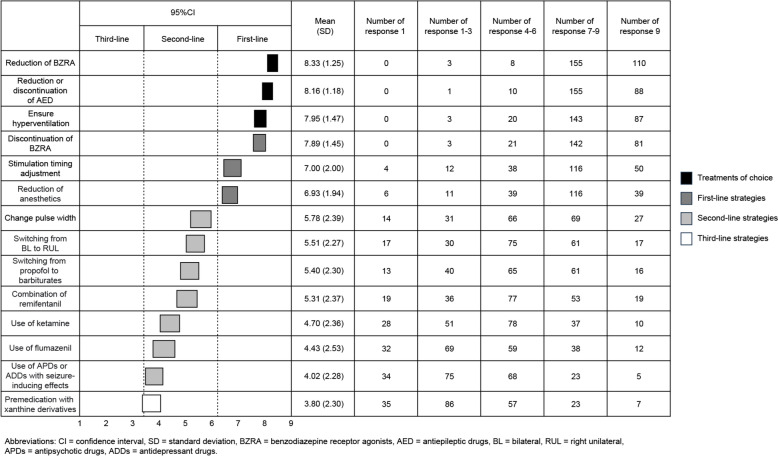
Methods: We asked Japanese ECT experts to rate 14 approaches under six conditions of DECs on a 9-point Likert scale (1 = "disagree" to 9 = "agree"). Based on responses from 195 experts, the approaches were classified as first-line (95% confidence interval mean ≥ 6.5), second-line (mean, 3.5-6.5), or third-line strategies (mean < 3.5). Approaches rated 9 points by at least 50% of the respondents were considered "treatments of choice."
Results: To avoid difficult seizure induction, dose reduction of benzodiazepine receptor agonist (BZRA) (8.33 ± 1.25), dose reduction or discontinuation of antiepileptic drugs (AEDs) or other drugs that may make seizure induction difficult (8.16 ± 1.18), and ensure hyperventilation (7.95 ± 1.47) were classified as treatments of choice. First-line treatment strategies were BRZA discontinuation (7.89 ± 1.45), stimulation timing adjustment (7.00 ± 2.00), and anesthetic dose reduction (6.93 ± 1.94). Dose reduction or discontinuation of AEDs or other drugs that might make seizure induction difficult and ensure hyperventilation were the treatments of choice across all patient conditions. The results of rating approaches for patients with mood disorders and schizophrenia were similar, with differences observed among the approaches for patients with catatonia, high risk of cognitive impairment, and cardiovascular events.
Conclusions: ECT expert recommendations are useful and can assist in clinical decision-making. Our results suggest that while some strategies are applicable across all conditions, others should be tailored to meet the specific needs of patients. These recommendations should be further evaluated in future clinical studies.
期刊介绍:
Annals of General Psychiatry considers manuscripts on all aspects of psychiatry, including neuroscience and psychological medicine. Both basic and clinical neuroscience contributions are encouraged.
Annals of General Psychiatry emphasizes a biopsychosocial approach to illness and health and strongly supports and follows the principles of evidence-based medicine. As an open access journal, Annals of General Psychiatry facilitates the worldwide distribution of high quality psychiatry and mental health research. The journal considers submissions on a wide range of topics including, but not limited to, psychopharmacology, forensic psychiatry, psychotic disorders, psychiatric genetics, and mood and anxiety disorders.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
