Resham Ramkissoon, Ashley Rosier, Savitha Iyengar, Timucin Taner, William Sanchez
{"title":"Improving 1-year liver allograft survival hazard ratios.","authors":"Resham Ramkissoon, Ashley Rosier, Savitha Iyengar, Timucin Taner, William Sanchez","doi":"10.1136/bmjoq-2024-002899","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Scientific Registry for Transplant Recipients (SRTR) publishes outcomes of all transplant centres in the USA two times a year. The outcomes are publicly available and used by insurance payers and patients to assess the performance of a programme. Poor performance can result in temporary suspension or termination of a transplant programme. The estimated 1-year survival hazard ratio (EHR) is an important metric publicly reported by the SRTR.</p><p><strong>Problem: </strong>The EHR at our institution was 1.13, indicating a graft loss rate that was 13% higher than the national average.</p><p><strong>Methods/intervention: </strong>We defined an improvement in this metric as achieving an EHR of <1.0. Our balance measure was maintaining similar liver transplant volumes and avoiding limiting access to transplant. Using a causality tree, we identified there was no 'real time' assessment of programme risk or objective metric to assess this. An affinity diagram was used to determine high and intermediate risk factors for mortality and graft loss and, using a REDCap form (a web application used to manage our database) to track actual and potential complications, we calculated a weekly 'risk metric' that was introduced at multidisciplinary selection conference meetings.</p><p><strong>Results: </strong>We remeasured our EHR at each interval release of the SRTR outcomes and found it to be 0.98 and 0.65 after implementing the 'risk metric.' During the intervention period, annual liver transplant volume remained above the baseline measure.</p><p><strong>Conclusion: </strong>By implementing a 'risk metric' to prospectively assess the risk of a low EHR at transplant selection committee meetings, we were able to reduce the EHR well below the national average without limiting access to liver transplants.</p>","PeriodicalId":9052,"journal":{"name":"BMJ Open Quality","volume":"14 1","pages":""},"PeriodicalIF":1.6000,"publicationDate":"2025-01-11","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11752011/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Open Quality","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjoq-2024-002899","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q4","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The Scientific Registry for Transplant Recipients (SRTR) publishes outcomes of all transplant centres in the USA two times a year. The outcomes are publicly available and used by insurance payers and patients to assess the performance of a programme. Poor performance can result in temporary suspension or termination of a transplant programme. The estimated 1-year survival hazard ratio (EHR) is an important metric publicly reported by the SRTR.
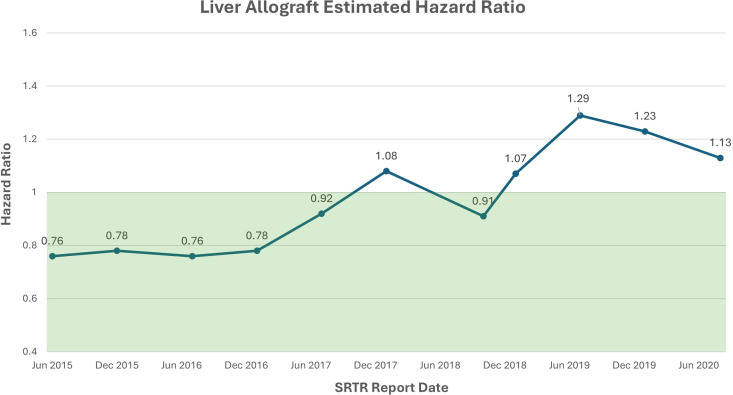
Problem: The EHR at our institution was 1.13, indicating a graft loss rate that was 13% higher than the national average.
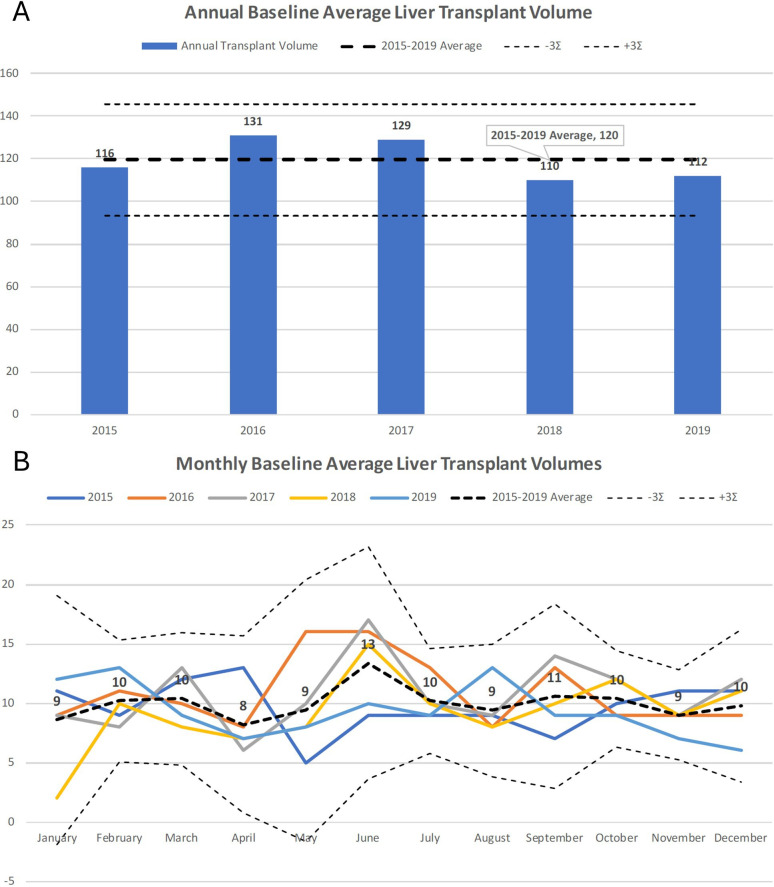
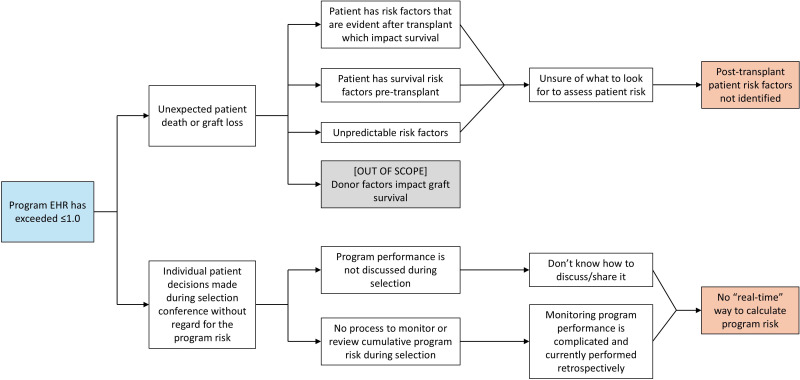
Methods/intervention: We defined an improvement in this metric as achieving an EHR of <1.0. Our balance measure was maintaining similar liver transplant volumes and avoiding limiting access to transplant. Using a causality tree, we identified there was no 'real time' assessment of programme risk or objective metric to assess this. An affinity diagram was used to determine high and intermediate risk factors for mortality and graft loss and, using a REDCap form (a web application used to manage our database) to track actual and potential complications, we calculated a weekly 'risk metric' that was introduced at multidisciplinary selection conference meetings.
Results: We remeasured our EHR at each interval release of the SRTR outcomes and found it to be 0.98 and 0.65 after implementing the 'risk metric.' During the intervention period, annual liver transplant volume remained above the baseline measure.
Conclusion: By implementing a 'risk metric' to prospectively assess the risk of a low EHR at transplant selection committee meetings, we were able to reduce the EHR well below the national average without limiting access to liver transplants.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
