{"title":"Treatment of Crohn's Disease With Infliximab and Subsequent Development of Takayasu's Arteritis.","authors":"Kei Nomura, Tomoyoshi Shibuya, Momoko Furusho, Hirotaka Ishino, Masayuki Orikasa, Masashi Omori, Rina Odakura, Masao Koma, Kentaro Ito, Takafumi Maruyama, Dai Ishikawa, Mariko Hojo, Akihito Nagahara","doi":"10.14740/gr1792","DOIUrl":null,"url":null,"abstract":"<p><p>A 23-year-old man was diagnosed with Crohn's disease (CD) of the large intestine after colonoscopy revealed longitudinal ulcers, and pathology revealed non-caseating epithelioid cell granulomas and anal fistulas. The CD relapsed, and therefore prednisolone (PSL) and infliximab (IFX) treatment was initiated. The PSL was gradually tapered. Steroid-free remission was maintained with IFX. The patient subsequently developed a high fever and headache, while CD-related symptoms did not worsen. Laboratory data showed white blood cells at 14,200/µL and C-reactive protein at 17.2 mg/dL. Contrast-enhanced computed tomography revealed thoracoabdominal aortitis, and the patient was consequently diagnosed with Takayasu's arteritis (TA). We therefore again initiated PSL treatment that immediately reduced the fever and headache. The PSL dose was again tapered and the administration of IFX was resumed to maintain CD remission. No further episodes of aortitis relapse were noted after restarting IFX, and the CD currently remains in remission. This is a rare case of TA onset during IFX treatment for CD, and, as such, contributes to the limited literature on such cases. More specifically, this case highlights that when patients with CD present with symptoms such as fever or headache, it is necessary to investigate the possibility of vasculitis.</p>","PeriodicalId":12461,"journal":{"name":"Gastroenterology Research","volume":"17 5-6","pages":"217-223"},"PeriodicalIF":1.7000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11711032/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gastroenterology Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14740/gr1792","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/12/28 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
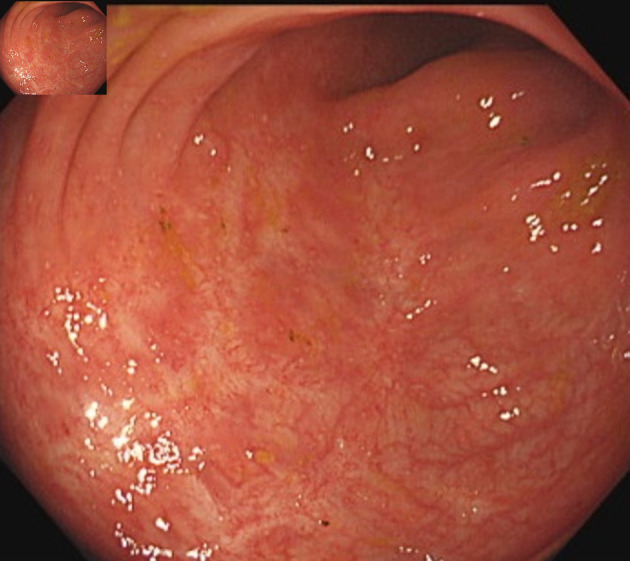
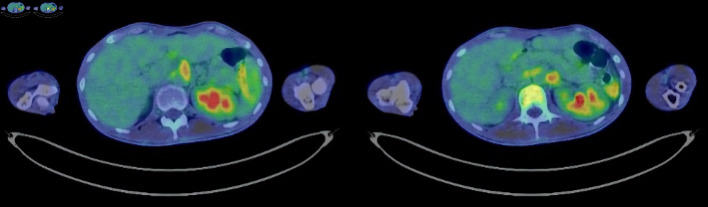
A 23-year-old man was diagnosed with Crohn's disease (CD) of the large intestine after colonoscopy revealed longitudinal ulcers, and pathology revealed non-caseating epithelioid cell granulomas and anal fistulas. The CD relapsed, and therefore prednisolone (PSL) and infliximab (IFX) treatment was initiated. The PSL was gradually tapered. Steroid-free remission was maintained with IFX. The patient subsequently developed a high fever and headache, while CD-related symptoms did not worsen. Laboratory data showed white blood cells at 14,200/µL and C-reactive protein at 17.2 mg/dL. Contrast-enhanced computed tomography revealed thoracoabdominal aortitis, and the patient was consequently diagnosed with Takayasu's arteritis (TA). We therefore again initiated PSL treatment that immediately reduced the fever and headache. The PSL dose was again tapered and the administration of IFX was resumed to maintain CD remission. No further episodes of aortitis relapse were noted after restarting IFX, and the CD currently remains in remission. This is a rare case of TA onset during IFX treatment for CD, and, as such, contributes to the limited literature on such cases. More specifically, this case highlights that when patients with CD present with symptoms such as fever or headache, it is necessary to investigate the possibility of vasculitis.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
