Tommi Bergman, Maija-Liisa Kalliomäki, Mika Särkelä, Jarkko Harju
{"title":"The use of the surgical pleth index to guide anaesthesia in gastroenterological surgery: a randomised controlled study.","authors":"Tommi Bergman, Maija-Liisa Kalliomäki, Mika Särkelä, Jarkko Harju","doi":"10.1007/s10877-025-01262-6","DOIUrl":null,"url":null,"abstract":"<p><p>The measurement of nociception and the optimisation of intraoperative antinociceptive medication could potentially improve the conduct of anaesthesia, especially in the older population. The Surgical Pleth Index (SPI) is one of the monitoring methods presently used for the detection of nociceptive stimulus. Eighty patients aged 50 years and older who were scheduled to undergo major abdominal surgery were randomised and divided into a study group and a control group. In the study group, the SPI was used to guide the administration of remifentanil during surgery. In the control group, the SPI value was concealed, and remifentanil administration was based on the clinical evaluation of the attending anaesthesiologist. The primary endpoint of this study was intraoperative remifentanil consumption. In addition, we compared the durations of intraoperative hypotension and hypertension. No difference in intraoperative remifentanil consumption (4.5 µg kg<sup>- 1</sup>h<sup>- 1</sup> vs. 5.6 µg kg<sup>- 1</sup>h<sup>- 1</sup>, p = 0.14) was found. Furthermore, there was no difference in the proportion of hypotensive time (mean arterial pressure, MAP < 65) (3.7% vs. 1.6%, p = 0.40). However, in the subgroup of patients who underwent operation with invasive blood pressure monitoring, there was less severe hypotension (MAP < 55) (0.3% vs. 0.0%, p = 0.02) and intermediate hypotension (MAP < 65) (10.2% vs. 2.6%, p = 0.07) in the treatment group, even though remifentanil consumption was higher (3.5 µg kg<sup>- 1</sup>h<sup>- 1</sup> vs. 5.1 µg kg<sup>- 1</sup>h<sup>- 1</sup>p = 0.03). The use of SPI guidance for the administration of remifentanil during surgery did not help to reduce the remifentanil consumption. However, the results from invasively monitored study group suggest more timely administered opioid when SPI was used.</p>","PeriodicalId":15513,"journal":{"name":"Journal of Clinical Monitoring and Computing","volume":" ","pages":"957-965"},"PeriodicalIF":2.2000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12474587/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Clinical Monitoring and Computing","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10877-025-01262-6","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/20 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
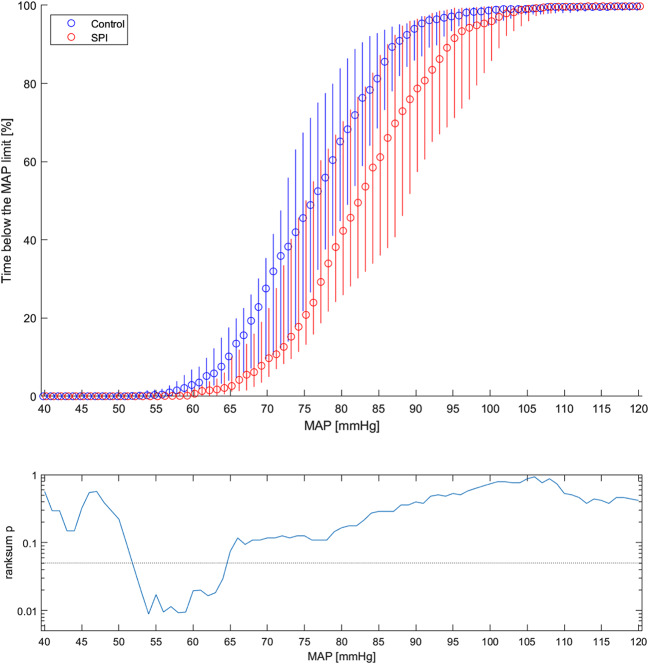
The measurement of nociception and the optimisation of intraoperative antinociceptive medication could potentially improve the conduct of anaesthesia, especially in the older population. The Surgical Pleth Index (SPI) is one of the monitoring methods presently used for the detection of nociceptive stimulus. Eighty patients aged 50 years and older who were scheduled to undergo major abdominal surgery were randomised and divided into a study group and a control group. In the study group, the SPI was used to guide the administration of remifentanil during surgery. In the control group, the SPI value was concealed, and remifentanil administration was based on the clinical evaluation of the attending anaesthesiologist. The primary endpoint of this study was intraoperative remifentanil consumption. In addition, we compared the durations of intraoperative hypotension and hypertension. No difference in intraoperative remifentanil consumption (4.5 µg kg- 1h- 1 vs. 5.6 µg kg- 1h- 1, p = 0.14) was found. Furthermore, there was no difference in the proportion of hypotensive time (mean arterial pressure, MAP < 65) (3.7% vs. 1.6%, p = 0.40). However, in the subgroup of patients who underwent operation with invasive blood pressure monitoring, there was less severe hypotension (MAP < 55) (0.3% vs. 0.0%, p = 0.02) and intermediate hypotension (MAP < 65) (10.2% vs. 2.6%, p = 0.07) in the treatment group, even though remifentanil consumption was higher (3.5 µg kg- 1h- 1 vs. 5.1 µg kg- 1h- 1p = 0.03). The use of SPI guidance for the administration of remifentanil during surgery did not help to reduce the remifentanil consumption. However, the results from invasively monitored study group suggest more timely administered opioid when SPI was used.
期刊介绍:
The Journal of Clinical Monitoring and Computing is a clinical journal publishing papers related to technology in the fields of anaesthesia, intensive care medicine, emergency medicine, and peri-operative medicine.
The journal has links with numerous specialist societies, including editorial board representatives from the European Society for Computing and Technology in Anaesthesia and Intensive Care (ESCTAIC), the Society for Technology in Anesthesia (STA), the Society for Complex Acute Illness (SCAI) and the NAVAt (NAVigating towards your Anaestheisa Targets) group.
The journal publishes original papers, narrative and systematic reviews, technological notes, letters to the editor, editorial or commentary papers, and policy statements or guidelines from national or international societies. The journal encourages debate on published papers and technology, including letters commenting on previous publications or technological concerns. The journal occasionally publishes special issues with technological or clinical themes, or reports and abstracts from scientificmeetings. Special issues proposals should be sent to the Editor-in-Chief. Specific details of types of papers, and the clinical and technological content of papers considered within scope can be found in instructions for authors.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
