Elliott M Sina, Somya Shankar, Maurits S Boon, Colin T Huntley
{"title":"Risk of Motor Vehicle Accidents in Obstructive Sleep Apnea: Comparative Analysis of CPAP Versus Surgery.","authors":"Elliott M Sina, Somya Shankar, Maurits S Boon, Colin T Huntley","doi":"10.1002/ohn.1131","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To compare the incidence of motor vehicle accidents (MVAs) among patients with obstructive sleep apnea (OSA) undergoing continuous positive airway pressure (CPAP) therapy and sleep surgery.</p><p><strong>Study design: </strong>Retrospective cohort study using the TriNetX national clinical database.</p><p><strong>Setting: </strong>Analysis of a nationwide patient cohort.</p><p><strong>Methods: </strong>The database was queried for patients with OSA (International Classification of Diseases, 10th Revision: G47.33) treated with CPAP (Current Procedural Terminology [CPT]: 94660), sleep surgery (CPT: 42145, 64568, 64582), or no treatment. Sleep surgeries included uvulopalatopharyngoplasty and hypoglossal nerve stimulation. 1:1 Propensity score matching (PSM) ensured cohort comparability by age, sex, and race. MVA incidence rates were analyzed, along with a subanalysis of OSA-related comorbidities as a surrogate of OSA severity.</p><p><strong>Results: </strong>A total of 2,832,437 patients with OSA were identified. Patients with OSA undergoing sleep surgery demonstrated a significantly lower incidence of MVAs (3.403%) compared to the OSA + CPAP cohort (6.072%) and the no-treatment group (4.662%). The odds ratio (OR) for MVA incidence in the no-treatment group compared to the OSA + sleep surgery cohort was 1.214 (95% confidence interval [CI]: 1.060-1.391, P = .0051). The OR in the OSA + sleep surgery cohort compared to the CPAP cohort was 0.545 (95% CI: 0.480-0.618, P < .0001). Patients with OSA who experienced MVAs were more likely to have comorbidities such as hypertension, diabetes, and heart failure following the accident.</p><p><strong>Conclusion: </strong>Sleep surgery significantly reduces the risk of MVAs in patients with OSA compared to CPAP and no treatment. In appropriate candidates, surgery should be considered to mitigate personal and public health risks associated with OSA.</p>","PeriodicalId":19707,"journal":{"name":"Otolaryngology- Head and Neck Surgery","volume":" ","pages":"1459-1467"},"PeriodicalIF":2.5000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11947857/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Otolaryngology- Head and Neck Surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ohn.1131","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: To compare the incidence of motor vehicle accidents (MVAs) among patients with obstructive sleep apnea (OSA) undergoing continuous positive airway pressure (CPAP) therapy and sleep surgery.
Study design: Retrospective cohort study using the TriNetX national clinical database.
Setting: Analysis of a nationwide patient cohort.
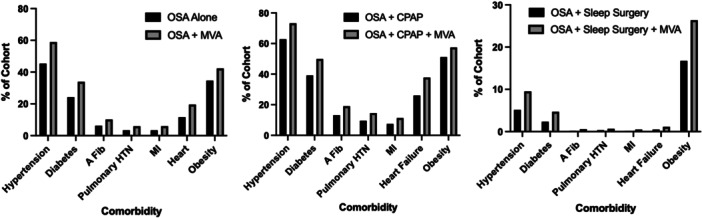
Methods: The database was queried for patients with OSA (International Classification of Diseases, 10th Revision: G47.33) treated with CPAP (Current Procedural Terminology [CPT]: 94660), sleep surgery (CPT: 42145, 64568, 64582), or no treatment. Sleep surgeries included uvulopalatopharyngoplasty and hypoglossal nerve stimulation. 1:1 Propensity score matching (PSM) ensured cohort comparability by age, sex, and race. MVA incidence rates were analyzed, along with a subanalysis of OSA-related comorbidities as a surrogate of OSA severity.
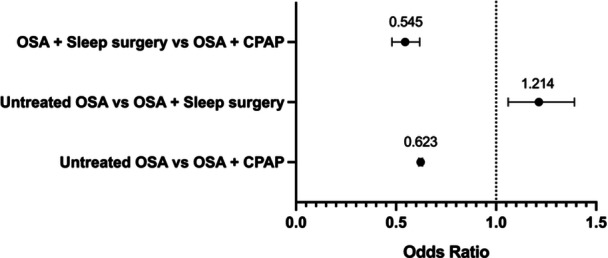
Results: A total of 2,832,437 patients with OSA were identified. Patients with OSA undergoing sleep surgery demonstrated a significantly lower incidence of MVAs (3.403%) compared to the OSA + CPAP cohort (6.072%) and the no-treatment group (4.662%). The odds ratio (OR) for MVA incidence in the no-treatment group compared to the OSA + sleep surgery cohort was 1.214 (95% confidence interval [CI]: 1.060-1.391, P = .0051). The OR in the OSA + sleep surgery cohort compared to the CPAP cohort was 0.545 (95% CI: 0.480-0.618, P < .0001). Patients with OSA who experienced MVAs were more likely to have comorbidities such as hypertension, diabetes, and heart failure following the accident.
Conclusion: Sleep surgery significantly reduces the risk of MVAs in patients with OSA compared to CPAP and no treatment. In appropriate candidates, surgery should be considered to mitigate personal and public health risks associated with OSA.
期刊介绍:
Otolaryngology–Head and Neck Surgery (OTO-HNS) is the official peer-reviewed publication of the American Academy of Otolaryngology–Head and Neck Surgery Foundation. The mission of Otolaryngology–Head and Neck Surgery is to publish contemporary, ethical, clinically relevant information in otolaryngology, head and neck surgery (ear, nose, throat, head, and neck disorders) that can be used by otolaryngologists, clinicians, scientists, and specialists to improve patient care and public health.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
