Pooja Budhiraja, Jesse D Schold, Rocio Lopez, Susana Arrigain, Bruce Kaplan
{"title":"Evaluating the impact of donor eGFR and HLA-DR mismatch on graft survival in living donor kidney transplants.","authors":"Pooja Budhiraja, Jesse D Schold, Rocio Lopez, Susana Arrigain, Bruce Kaplan","doi":"10.3389/fneph.2024.1518791","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study assesses the impact of human leukocyte antigen (HLA)-DR mismatch and donor-estimated glomerular filtration rate (eGFR) on outcomes of living donor kidney transplantation (LDKT), which are especially relevant to the availability of multiple donors and paired kidney exchanges.</p><p><strong>Methods: </strong>Using data from the Scientific Registry of Transplant Recipients (SRTR), we retrospectively analyzed graft survival in adult LDKT recipients transplanted between January 2013 and September 2022. Recipients with 0 HLA-DR mismatches were compared to those with 1-2 HLA-DR mismatches. Cox models assessed the association between donor eGFR and graft and patient survival, stratifying by a) HLA-DR mismatches, and b) HLA-DR mismatches and recipient age.</p><p><strong>Results: </strong>Among 44,080 recipients, 7,195 had 0 HLA-DR mismatches and 36,885 had 1-2 HLA-DR mismatches. The recipients' mean age was 49.1 for the 0 HLA-DR mismatch group and 50.4 for the 1-2 HLA-DR mismatch group. The donors' mean age was 43.1 and 43.8, with an eGFR of 101.0 and 99.9 ml/min, respectively. A higher donor eGFR was associated with better graft survival. Stratified analyses showed higher donor eGFR levels reduced the risk of graft loss in cases with DR mismatch (p < 0.001) but not in cases without HLA-DR mismatch (p = 0.81). This effect was significant for recipients aged 18-39 and over 60. Similar results were observed for patient survival.</p><p><strong>Conclusions: </strong>Higher donor eGFR was associated with lower risks of graft loss and patient death in the HLA-DR mismatch group but not the 0 HLA-DR mismatch group. These results emphasize the importance of considering both HLA-DR matching and donor kidney function, particularly for younger recipients to avoid sensitization for future transplants.</p>","PeriodicalId":73091,"journal":{"name":"Frontiers in nephrology","volume":"4 ","pages":"1518791"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11747204/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in nephrology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/fneph.2024.1518791","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study assesses the impact of human leukocyte antigen (HLA)-DR mismatch and donor-estimated glomerular filtration rate (eGFR) on outcomes of living donor kidney transplantation (LDKT), which are especially relevant to the availability of multiple donors and paired kidney exchanges.
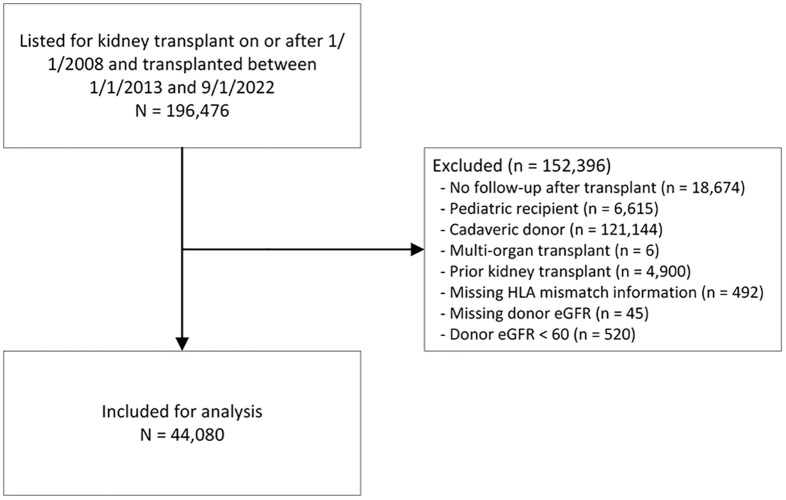
Methods: Using data from the Scientific Registry of Transplant Recipients (SRTR), we retrospectively analyzed graft survival in adult LDKT recipients transplanted between January 2013 and September 2022. Recipients with 0 HLA-DR mismatches were compared to those with 1-2 HLA-DR mismatches. Cox models assessed the association between donor eGFR and graft and patient survival, stratifying by a) HLA-DR mismatches, and b) HLA-DR mismatches and recipient age.
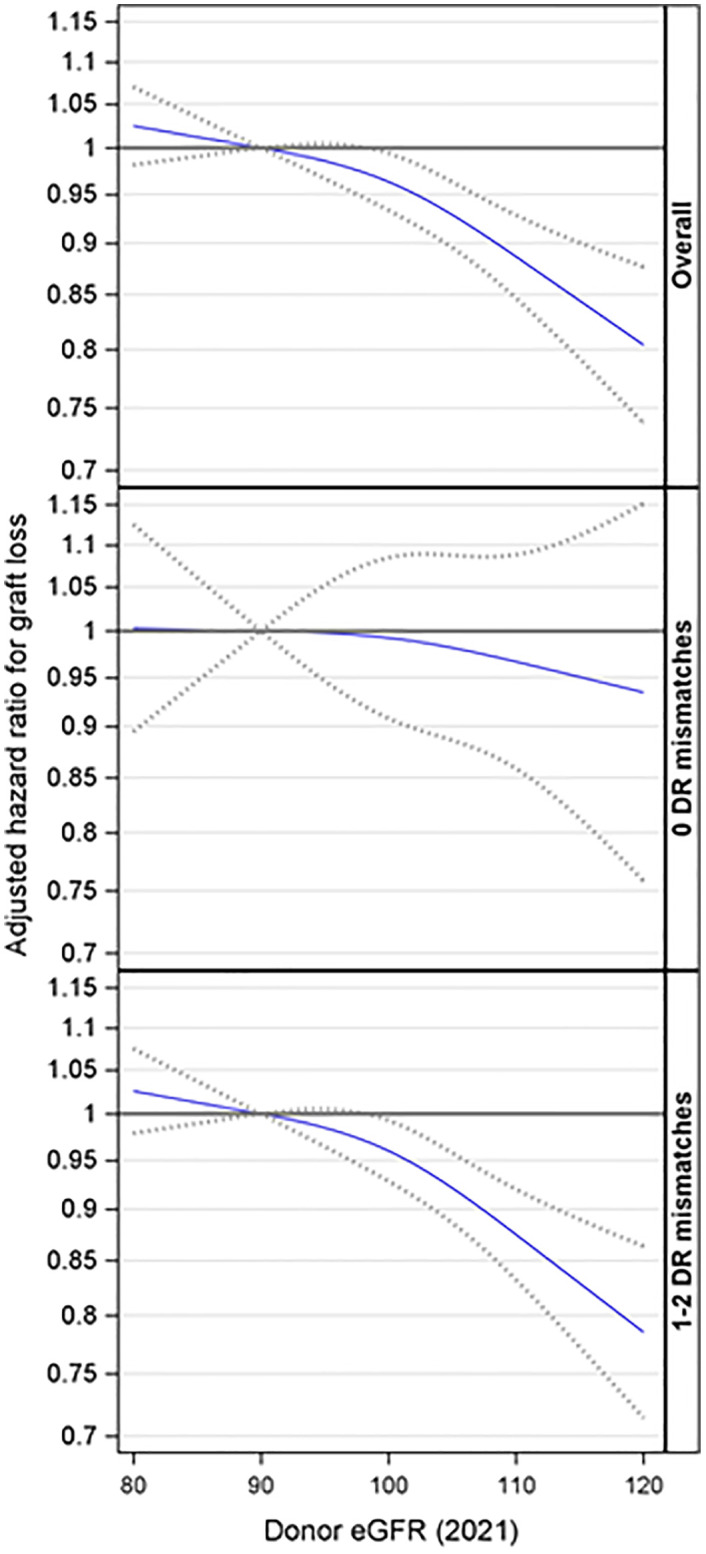
Results: Among 44,080 recipients, 7,195 had 0 HLA-DR mismatches and 36,885 had 1-2 HLA-DR mismatches. The recipients' mean age was 49.1 for the 0 HLA-DR mismatch group and 50.4 for the 1-2 HLA-DR mismatch group. The donors' mean age was 43.1 and 43.8, with an eGFR of 101.0 and 99.9 ml/min, respectively. A higher donor eGFR was associated with better graft survival. Stratified analyses showed higher donor eGFR levels reduced the risk of graft loss in cases with DR mismatch (p < 0.001) but not in cases without HLA-DR mismatch (p = 0.81). This effect was significant for recipients aged 18-39 and over 60. Similar results were observed for patient survival.
Conclusions: Higher donor eGFR was associated with lower risks of graft loss and patient death in the HLA-DR mismatch group but not the 0 HLA-DR mismatch group. These results emphasize the importance of considering both HLA-DR matching and donor kidney function, particularly for younger recipients to avoid sensitization for future transplants.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
