Álmos Schranc, Roberta Südy, John Daniels, Fabienne Fontao, Ferenc Peták, Walid Habre, Gergely Albu
{"title":"Effects of Variable Ventilation on Gas Exchange in an Experimental Model of Capnoperitoneum: A Randomized Crossover Study.","authors":"Álmos Schranc, Roberta Südy, John Daniels, Fabienne Fontao, Ferenc Peták, Walid Habre, Gergely Albu","doi":"10.1213/ANE.0000000000007418","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The rapid advancement of minimally invasive surgical techniques has made laparoscopy a preferred alternative because it reduces postoperative complications. However, inflating the peritoneum with CO 2 causes a cranial shift of the diaphragm decreasing lung volume and impairing gas exchange. Additionally, CO 2 absorption increases blood CO 2 levels, further complicating mechanical ventilation when the lung function is already compromised. Standard interventions such as lung recruitment maneuvers or increasing positive end-expiratory pressures can counteract these effects but also increase lung parenchymal strain and intrathoracic pressure, negatively impacting cardiac output. The application of variability in tidal volume and respiratory rate during mechanical ventilation to mimic natural breathing has shown benefits in various respiratory conditions. Therefore, we aimed to evaluate the short-term benefits of variable ventilation (VV) on gas exchange, respiratory mechanics, and hemodynamics during and after capnoperitoneum, compared to conventional pressure-controlled ventilation (PCV).</p><p><strong>Methods: </strong>Eleven anaesthetized rabbits were randomly assigned to PCV or VV. Oxygenation index (Pa o2 /FiO 2 ), arterial partial pressure of carbon dioxide (Pa co2 ), and respiratory mechanical parameters were assessed after a 15-minute-long ventilation period before, during, and after capnoperitoneum. According to a crossover design, after measurements at the 3 different stages, the ventilation mode was changed, and the entire sequence was repeated.</p><p><strong>Results: </strong>Capnoperitoneum compromised respiratory mechanics, decreased oxygenation, and caused CO 2 -retention compared to baseline measurements under both ventilation modalities ( P < .05, for all). Application of VV resulted in lower Pa o2 /FiO 2 (405. 5 ± 34.1 (mean ± standard deviation [SD]) vs 370. 5 ± 44.9, P < .001) and higher Pa co2 (48. 4 ± 5.1 vs 52. 8 ± 6.0 mm Hg, P = .009) values during capnoperitoneum compared to PCV. After abdominal deflation and a lung recruitment maneuver, VV proved more beneficial for CO 2 removal than PCV (41. 0 ± 2.3 vs 44. 6 ± 4.3mmHg, P = .027). No significant difference was observed in the respiratory mechanical or hemodynamic parameters between the ventilation modalities under the same conditions.</p><p><strong>Conclusions: </strong>The detrimental effects of capnoperitoneum on gas exchange were more pronounced with VV. However, after the release of capnoperitoneum, VV significantly improved CO 2 clearance. Therefore, VV could possibly be considered as an alternative ventilation modality to restore physiological gas exchange after, but not during, capnoperitoneum.</p>","PeriodicalId":7784,"journal":{"name":"Anesthesia and analgesia","volume":" ","pages":"1159-1167"},"PeriodicalIF":3.8000,"publicationDate":"2025-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12509449/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Anesthesia and analgesia","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1213/ANE.0000000000007418","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/22 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The rapid advancement of minimally invasive surgical techniques has made laparoscopy a preferred alternative because it reduces postoperative complications. However, inflating the peritoneum with CO 2 causes a cranial shift of the diaphragm decreasing lung volume and impairing gas exchange. Additionally, CO 2 absorption increases blood CO 2 levels, further complicating mechanical ventilation when the lung function is already compromised. Standard interventions such as lung recruitment maneuvers or increasing positive end-expiratory pressures can counteract these effects but also increase lung parenchymal strain and intrathoracic pressure, negatively impacting cardiac output. The application of variability in tidal volume and respiratory rate during mechanical ventilation to mimic natural breathing has shown benefits in various respiratory conditions. Therefore, we aimed to evaluate the short-term benefits of variable ventilation (VV) on gas exchange, respiratory mechanics, and hemodynamics during and after capnoperitoneum, compared to conventional pressure-controlled ventilation (PCV).
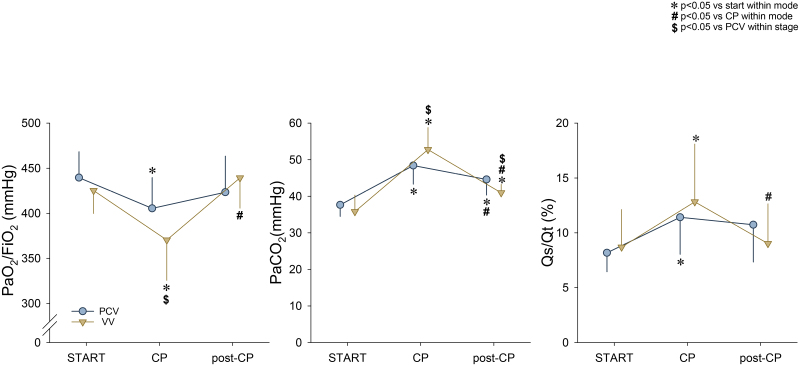
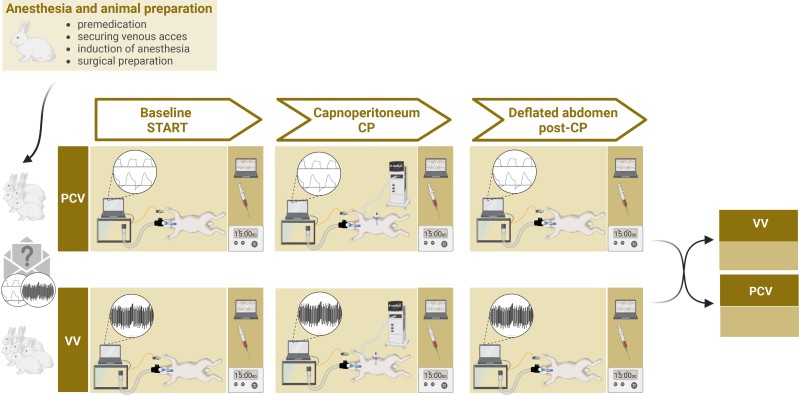
Methods: Eleven anaesthetized rabbits were randomly assigned to PCV or VV. Oxygenation index (Pa o2 /FiO 2 ), arterial partial pressure of carbon dioxide (Pa co2 ), and respiratory mechanical parameters were assessed after a 15-minute-long ventilation period before, during, and after capnoperitoneum. According to a crossover design, after measurements at the 3 different stages, the ventilation mode was changed, and the entire sequence was repeated.
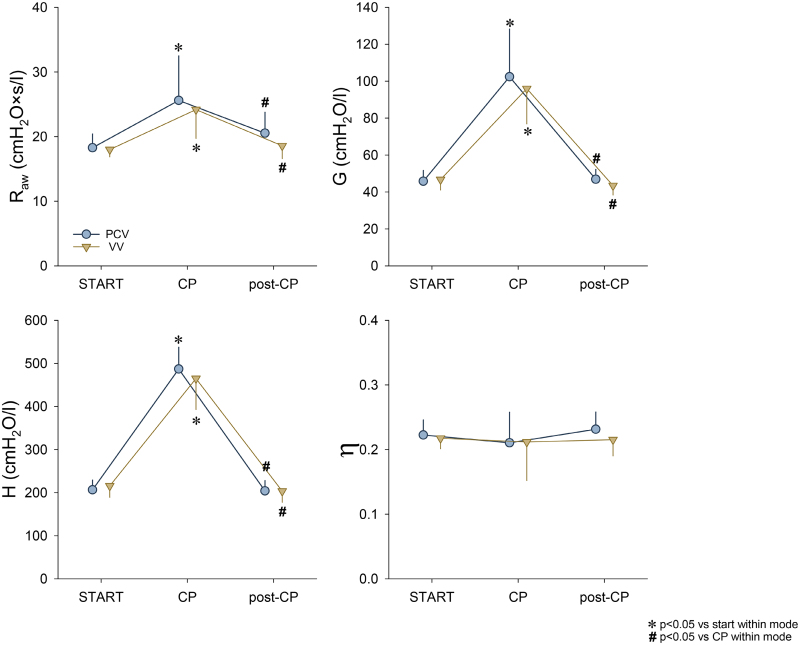
Results: Capnoperitoneum compromised respiratory mechanics, decreased oxygenation, and caused CO 2 -retention compared to baseline measurements under both ventilation modalities ( P < .05, for all). Application of VV resulted in lower Pa o2 /FiO 2 (405. 5 ± 34.1 (mean ± standard deviation [SD]) vs 370. 5 ± 44.9, P < .001) and higher Pa co2 (48. 4 ± 5.1 vs 52. 8 ± 6.0 mm Hg, P = .009) values during capnoperitoneum compared to PCV. After abdominal deflation and a lung recruitment maneuver, VV proved more beneficial for CO 2 removal than PCV (41. 0 ± 2.3 vs 44. 6 ± 4.3mmHg, P = .027). No significant difference was observed in the respiratory mechanical or hemodynamic parameters between the ventilation modalities under the same conditions.
Conclusions: The detrimental effects of capnoperitoneum on gas exchange were more pronounced with VV. However, after the release of capnoperitoneum, VV significantly improved CO 2 clearance. Therefore, VV could possibly be considered as an alternative ventilation modality to restore physiological gas exchange after, but not during, capnoperitoneum.
背景:微创手术技术的快速发展使腹腔镜手术成为首选选择,因为它减少了术后并发症。然而,向腹膜充入二氧化碳会导致横膈膜的头部移位,减少肺容量并损害气体交换。此外,二氧化碳的吸收增加了血液中的二氧化碳水平,在肺功能已经受损的情况下,使机械通气进一步复杂化。标准干预措施,如肺复吸或增加呼气末正压可以抵消这些影响,但也会增加肺实质张力和胸内压,对心输出量产生负面影响。在机械通气过程中应用潮汐量和呼吸频率的变化来模拟自然呼吸,在各种呼吸条件下显示出益处。因此,我们旨在评估与常规压力控制通气(PCV)相比,可变通气(VV)在腹膜前后的气体交换、呼吸力学和血流动力学方面的短期益处。方法:11只麻醉兔随机分为PCV组和VV组。在腹膜前、腹膜中、腹膜后各15分钟通气后,评估氧合指数(Pao2/FiO2)、动脉二氧化碳分压(Paco2)及呼吸力学参数。根据交叉设计,在3个不同阶段测量后,改变通风方式,并重复整个顺序。结果:与两种通气方式下的基线测量结果相比,钙腹膜损害呼吸力学,降低氧合,并引起二氧化碳潴留(P < 0.05)。VV的应用降低了Pao2/FiO2(405)。5±34.1(平均值±标准差[SD]) vs 370。(5±44.9,P < 0.001), Paco2升高(48。4±5.1 vs 52。8±6.0 mm Hg, P = 0.009)。经腹部放气和肺部复吸后,VV比PCV更有利于CO2的去除(41)。0±2.3 vs 44。6±4.3mmHg, P = 0.027)。在相同条件下,两种通气方式的呼吸力学和血流动力学参数无显著差异。结论:腹膜对VV患者气体交换的不良影响更为明显。然而,在释放腹膜后,VV显著提高CO2清除率。因此,VV可能被认为是一种替代的通气方式,可以在腹膜后恢复生理气体交换,而不是在腹膜过程中。
期刊介绍:
Anesthesia & Analgesia exists for the benefit of patients under the care of health care professionals engaged in the disciplines broadly related to anesthesiology, perioperative medicine, critical care medicine, and pain medicine. The Journal furthers the care of these patients by reporting the fundamental advances in the science of these clinical disciplines and by documenting the clinical, laboratory, and administrative advances that guide therapy. Anesthesia & Analgesia seeks a balance between definitive clinical and management investigations and outstanding basic scientific reports. The Journal welcomes original manuscripts containing rigorous design and analysis, even if unusual in their approach.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
