{"title":"Predicting the onset of chronic kidney disease (CKD) for diabetic patients with aggregated longitudinal EMR data.","authors":"Neda Aminnejad, Michelle Greiver, Huaxiong Huang","doi":"10.1371/journal.pdig.0000700","DOIUrl":null,"url":null,"abstract":"<p><p>Chronic kidney disease (CKD) affects over 13% of the population, totaling more than 800 million individuals worldwide. Timely identification and intervention are crucial to delay CKD progression and improve patient outcomes. This research focuses on developing a predictive model to classify diabetic patients showing signs of kidney function impairment based on their CKD development risk. Our model utilizes electronic medical record (EMR) data, specifically by incorporating patient demographics, laboratory results, chronic conditions, risk factors, and medication codes to predict the onset of CKD in diabetic patients six months in advance, achieving an average Area Under the Curve (AUC) of 0.88. We leverage aggregated EMR data to effectively capture relevant information within the observation year instead of using temporal EMR data. Furthermore, we identify the most significant features for predicting CKD onset, including mean, minimum, and first quartile of estimated glomerular filtration rate (eGFR) during the observation year, along with variables such as diagnosis age and duration of hypertension, osteoarthritis, and diabetes, as well as levels of hemoglobin and fasting blood glucose (FBG). We also explored a refined model utilizing only these most significant features, which yields a slightly lower AUC of 0.86. These variables are typically available in primary data, empowering physicians for real-time risk assessment. The proposed model's ability to identify higher-risk patients is essential for timely intervention, personalized care, risk stratification, patient education, and potential cost savings. This research contributes valuable insights for healthcare practitioners seeking efficient tools for early CKD detection in diabetic populations.</p>","PeriodicalId":74465,"journal":{"name":"PLOS digital health","volume":"4 1","pages":"e0000700"},"PeriodicalIF":7.7000,"publicationDate":"2025-01-22","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11753645/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PLOS digital health","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1371/journal.pdig.0000700","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
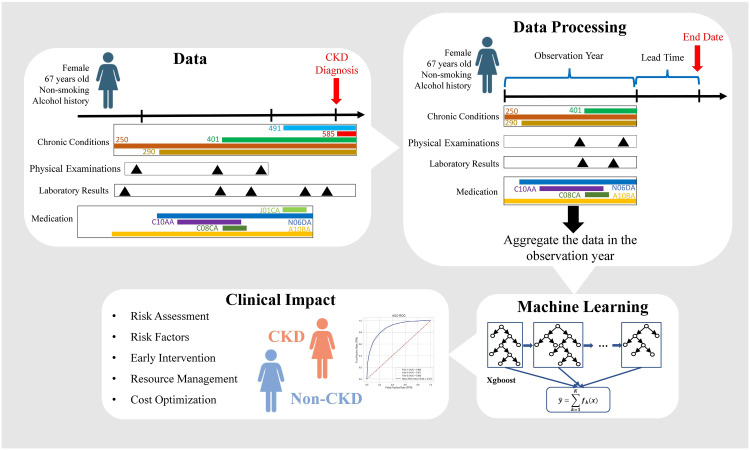
Chronic kidney disease (CKD) affects over 13% of the population, totaling more than 800 million individuals worldwide. Timely identification and intervention are crucial to delay CKD progression and improve patient outcomes. This research focuses on developing a predictive model to classify diabetic patients showing signs of kidney function impairment based on their CKD development risk. Our model utilizes electronic medical record (EMR) data, specifically by incorporating patient demographics, laboratory results, chronic conditions, risk factors, and medication codes to predict the onset of CKD in diabetic patients six months in advance, achieving an average Area Under the Curve (AUC) of 0.88. We leverage aggregated EMR data to effectively capture relevant information within the observation year instead of using temporal EMR data. Furthermore, we identify the most significant features for predicting CKD onset, including mean, minimum, and first quartile of estimated glomerular filtration rate (eGFR) during the observation year, along with variables such as diagnosis age and duration of hypertension, osteoarthritis, and diabetes, as well as levels of hemoglobin and fasting blood glucose (FBG). We also explored a refined model utilizing only these most significant features, which yields a slightly lower AUC of 0.86. These variables are typically available in primary data, empowering physicians for real-time risk assessment. The proposed model's ability to identify higher-risk patients is essential for timely intervention, personalized care, risk stratification, patient education, and potential cost savings. This research contributes valuable insights for healthcare practitioners seeking efficient tools for early CKD detection in diabetic populations.



 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
