Bridging thrombolysis with tenecteplase versus endovascular thrombectomy alone for large-vessel anterior circulation stroke: a target trial emulation analysis.
Valerian L Altersberger, Johannes Kaesmacher, Leonid Churilov, Vignan Yogendrakumar, Jan Gralla, Daniel Strbian, David J Seiffge, Peter J Mitchell, Timothy J Kleinig, Bruce Cv Campbell, Urs Fischer
{"title":"Bridging thrombolysis with tenecteplase versus endovascular thrombectomy alone for large-vessel anterior circulation stroke: a target trial emulation analysis.","authors":"Valerian L Altersberger, Johannes Kaesmacher, Leonid Churilov, Vignan Yogendrakumar, Jan Gralla, Daniel Strbian, David J Seiffge, Peter J Mitchell, Timothy J Kleinig, Bruce Cv Campbell, Urs Fischer","doi":"10.1136/jnnp-2024-335325","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Whether bridging thrombolysis with tenecteplase is beneficial compared with thrombectomy alone in patients who had a stroke with large-vessel occlusion remains unclear.</p><p><strong>Methods: </strong>This is a causal inference study of observational data from the trials SWIFT DIRECT and EXTEND-IA TNK Parts 1 and 2 applying target trial emulation. We compared patients receiving thrombectomy alone to patients receiving tenecteplase 0.25 mg/kg or 0.40 mg/kg before thrombectomy. The primary outcome was functional independence (modified Rankin Scale (mRS) of 0-2) at 90 days. Secondary outcomes included improvement over the full ordinal mRS scale, freedom of disability (mRS 0-1), mortality and occurrence of symptomatic intracranial haemorrhage. The average causal treatment effect was estimated via inverse probability of treatment weighting and G-Computation. We calculated standardised risk differences (SRDs) and adjusted (common) ORs (a(c)ORs).</p><p><strong>Results: </strong>Of 377 patients included in the target trial, 187 received thrombectomy alone and 190 tenecteplase before thrombectomy. Tenecteplase before thrombectomy did not increase the probability of patients achieving functional independence (SRD 0.04 (95% CI -0.06 to 0.13)) but resulted in a significant improvement in the mRS overall (acOR 1.56 (95% CI 1.07 to 2.23)) and in a higher probability of freedom from disability (SRD 0.10 (95% CI 0.01 to 0.20)). The probability for improvement of functional outcomes was further increased in patients treated within 140 min after onset (ordinal mRS acOR 1.63 (95% CI 1.04 to 2.56)). No significant differences in safety outcomes were observed between the two groups.</p><p><strong>Conclusion: </strong>Tenecteplase before thrombectomy compared with thrombectomy alone did not increase the probability of functional independence but resulted in significant improvement over the full mRS scale. This improvement was most evident in patients treated early.</p>","PeriodicalId":16418,"journal":{"name":"Journal of Neurology, Neurosurgery, and Psychiatry","volume":" ","pages":"775-783"},"PeriodicalIF":7.5000,"publicationDate":"2025-07-16","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12322409/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Neurology, Neurosurgery, and Psychiatry","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1136/jnnp-2024-335325","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Whether bridging thrombolysis with tenecteplase is beneficial compared with thrombectomy alone in patients who had a stroke with large-vessel occlusion remains unclear.
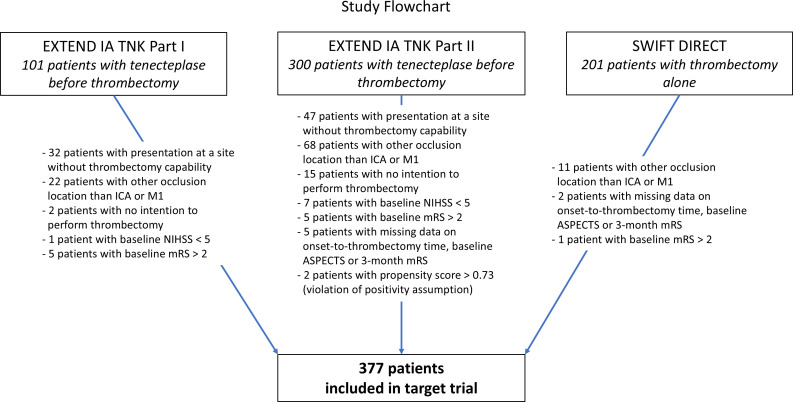
Methods: This is a causal inference study of observational data from the trials SWIFT DIRECT and EXTEND-IA TNK Parts 1 and 2 applying target trial emulation. We compared patients receiving thrombectomy alone to patients receiving tenecteplase 0.25 mg/kg or 0.40 mg/kg before thrombectomy. The primary outcome was functional independence (modified Rankin Scale (mRS) of 0-2) at 90 days. Secondary outcomes included improvement over the full ordinal mRS scale, freedom of disability (mRS 0-1), mortality and occurrence of symptomatic intracranial haemorrhage. The average causal treatment effect was estimated via inverse probability of treatment weighting and G-Computation. We calculated standardised risk differences (SRDs) and adjusted (common) ORs (a(c)ORs).
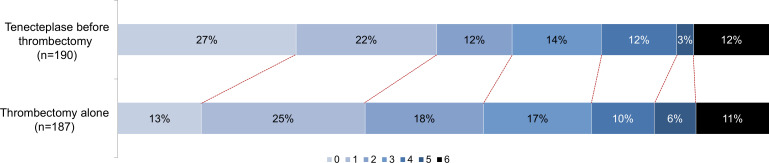
Results: Of 377 patients included in the target trial, 187 received thrombectomy alone and 190 tenecteplase before thrombectomy. Tenecteplase before thrombectomy did not increase the probability of patients achieving functional independence (SRD 0.04 (95% CI -0.06 to 0.13)) but resulted in a significant improvement in the mRS overall (acOR 1.56 (95% CI 1.07 to 2.23)) and in a higher probability of freedom from disability (SRD 0.10 (95% CI 0.01 to 0.20)). The probability for improvement of functional outcomes was further increased in patients treated within 140 min after onset (ordinal mRS acOR 1.63 (95% CI 1.04 to 2.56)). No significant differences in safety outcomes were observed between the two groups.
Conclusion: Tenecteplase before thrombectomy compared with thrombectomy alone did not increase the probability of functional independence but resulted in significant improvement over the full mRS scale. This improvement was most evident in patients treated early.
期刊介绍:
The Journal of Neurology, Neurosurgery & Psychiatry (JNNP) aspires to publish groundbreaking and cutting-edge research worldwide. Covering the entire spectrum of neurological sciences, the journal focuses on common disorders like stroke, multiple sclerosis, Parkinson’s disease, epilepsy, peripheral neuropathy, subarachnoid haemorrhage, and neuropsychiatry, while also addressing complex challenges such as ALS. With early online publication, regular podcasts, and an extensive archive collection boasting the longest half-life in clinical neuroscience journals, JNNP aims to be a trailblazer in the field.


 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
