Yulin Feng, Yinghua Lv, Juan Yang, Ling Xu, Junchao Chen, Jihan Huang, Jiyuan Ren, Qingshan Zheng, Lujin Li
{"title":"Quantitative evaluation of multiple treatment regimens for treatment-resistant depression.","authors":"Yulin Feng, Yinghua Lv, Juan Yang, Ling Xu, Junchao Chen, Jihan Huang, Jiyuan Ren, Qingshan Zheng, Lujin Li","doi":"10.1093/ijnp/pyaf007","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aims to quantitatively evaluate the efficacy and safety of various treatment regimens for treatment-resistant depression (TRD) across oral, intravenous, and intranasal routes to inform clinical guidelines.</p><p><strong>Methods: </strong>A systematic review identified randomized controlled trials on TRD, with efficacy measured by changes in the Montgomery-Åsberg Depression Rating Scale (MADRS). We developed pharmacodynamic and covariate models for different administration routes, using Monte Carlo simulations to estimate efficacy distribution. Dropout and adverse event-related dropout rates were analyzed via single-arm meta-analysis.</p><p><strong>Results: </strong>Involving 22 studies with 56 treatment arms and 3059 patients, our findings suggest combination therapies outperform monotherapy, achieving an additional 6.5% reduction in MADRS scores over 12 weeks. The most effective combinations were olanzapine with fluoxetine and quetiapine with selective serotonin reuptake inhibitors/ selective serotonin and norepinephrine reuptake inhibitors. Injectable treatments, particularly ayahuasca, produced rapid effects, with a 77% reduction in MADRS scores at 15 days. Intranasal treatments reached efficacy sooner than oral ones, with 28-day efficacy similar to the 12-week efficacy of the olanzapine-fluoxetine combination. Dropout rates due to adverse events were similar across methods (4.5%-5.2%), but total dropouts were highest for oral (17.9%) and lowest for intranasal routes (10.6%). Additionally, there was considerable variation in the incidence of headache, dizziness, and nausea across different administration routes.</p><p><strong>Conclusions: </strong>The quantitative evaluation of 22 TRD treatments illuminates key pharmacodynamic parameters, bolstering the development of clinical guidelines and aiding the design of clinical trials and medical decision-making.</p>","PeriodicalId":14134,"journal":{"name":"International Journal of Neuropsychopharmacology","volume":" ","pages":""},"PeriodicalIF":3.7000,"publicationDate":"2025-02-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11879141/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Neuropsychopharmacology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ijnp/pyaf007","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study aims to quantitatively evaluate the efficacy and safety of various treatment regimens for treatment-resistant depression (TRD) across oral, intravenous, and intranasal routes to inform clinical guidelines.
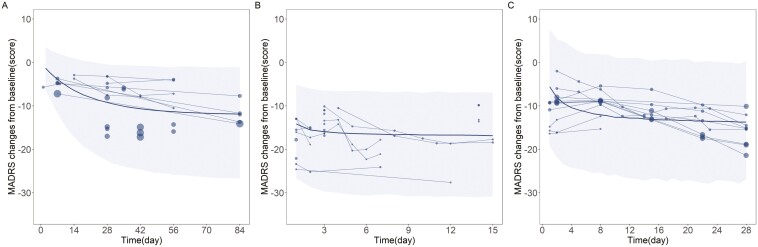
Methods: A systematic review identified randomized controlled trials on TRD, with efficacy measured by changes in the Montgomery-Åsberg Depression Rating Scale (MADRS). We developed pharmacodynamic and covariate models for different administration routes, using Monte Carlo simulations to estimate efficacy distribution. Dropout and adverse event-related dropout rates were analyzed via single-arm meta-analysis.
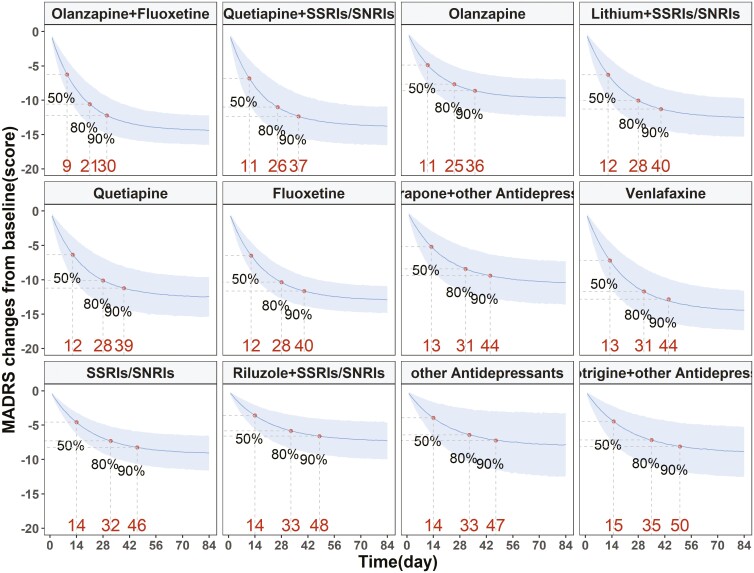
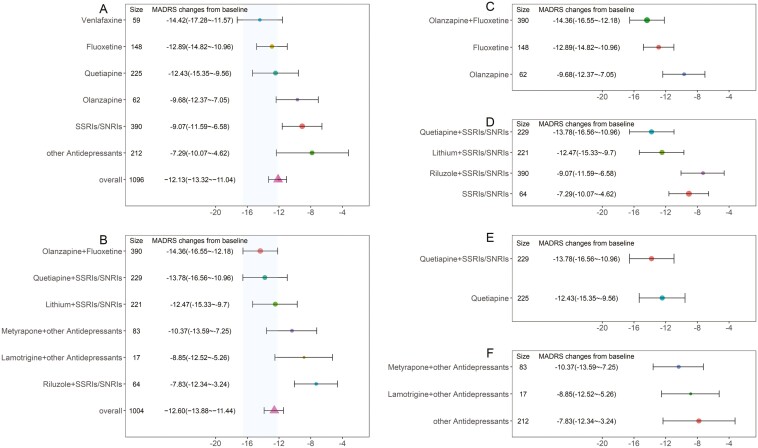
Results: Involving 22 studies with 56 treatment arms and 3059 patients, our findings suggest combination therapies outperform monotherapy, achieving an additional 6.5% reduction in MADRS scores over 12 weeks. The most effective combinations were olanzapine with fluoxetine and quetiapine with selective serotonin reuptake inhibitors/ selective serotonin and norepinephrine reuptake inhibitors. Injectable treatments, particularly ayahuasca, produced rapid effects, with a 77% reduction in MADRS scores at 15 days. Intranasal treatments reached efficacy sooner than oral ones, with 28-day efficacy similar to the 12-week efficacy of the olanzapine-fluoxetine combination. Dropout rates due to adverse events were similar across methods (4.5%-5.2%), but total dropouts were highest for oral (17.9%) and lowest for intranasal routes (10.6%). Additionally, there was considerable variation in the incidence of headache, dizziness, and nausea across different administration routes.
Conclusions: The quantitative evaluation of 22 TRD treatments illuminates key pharmacodynamic parameters, bolstering the development of clinical guidelines and aiding the design of clinical trials and medical decision-making.
期刊介绍:
The central focus of the journal is on research that advances understanding of existing and new neuropsychopharmacological agents including their mode of action and clinical application or provides insights into the biological basis of psychiatric disorders and thereby advances their pharmacological treatment. Such research may derive from the full spectrum of biological and psychological fields of inquiry encompassing classical and novel techniques in neuropsychopharmacology as well as strategies such as neuroimaging, genetics, psychoneuroendocrinology and neuropsychology.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
