Megan Othus, Guillermo Garcia-Manero, Frederick R. Appelbaum, Harry P. Erba, Eliana Dietrich, Suravi Raychaudhuri, Jacob Appelbaum, Elihu Estey, Mary-Elizabeth Percival
{"title":"Probability of remission with reinduction with 7+3 versus high-dose cytarabine: analysis of SWOG trial S1203","authors":"Megan Othus, Guillermo Garcia-Manero, Frederick R. Appelbaum, Harry P. Erba, Eliana Dietrich, Suravi Raychaudhuri, Jacob Appelbaum, Elihu Estey, Mary-Elizabeth Percival","doi":"10.1038/s41375-024-02512-3","DOIUrl":null,"url":null,"abstract":"","PeriodicalId":18109,"journal":{"name":"Leukemia","volume":"39 3","pages":"752-754"},"PeriodicalIF":13.4000,"publicationDate":"2025-01-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Leukemia","FirstCategoryId":"3","ListUrlMain":"https://www.nature.com/articles/s41375-024-02512-3","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"HEMATOLOGY","Score":null,"Total":0}
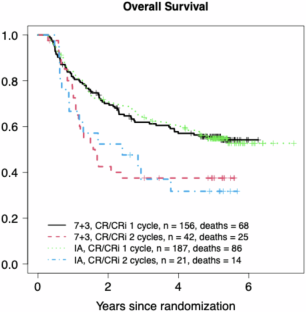
在急性髓性白血病(AML)患者中,强化诱导化疗的目标是诱导形态学上的完全缓解(分别有或没有计数恢复,CR或CRi),这与总生存期(OS)密切相关[1,2]。强化化疗被定义为标准的7+3方案或方案,使用阿糖胞苷,每日剂量≥1g /m2(如FLAG-ida, CLAG-M,或高剂量阿糖胞苷联合阿糖胞苷,称为IA)。一个常见的临床问题是,在第一个诱导疗程后疾病未达到CR的患者是否应该接受第二个相同的疗程或改变为不同的(通常是研究性的)方案bbb。由于后者的结果根据定义是未知的,因此必须根据第二疗程7+3或高剂量含阿糖胞苷方案的预期结果来决定。通过分析1980年代、1990年代和2000年代进行的SWOG试验S8600、S9031、S9333和S0106,我们之前报道的CR率为44% among 242 patients given a second course of 7+3 after failure of a first, compared to a CR rate of 48% among the 987 patients who received a first course [4]. Notably, in the most recent of these studies (S0106), though CR was still achieved in a high percentage of patients, survival was considerably longer if CR was observed after the first course [5]. In contrast to the similar rate of CR after the first or second course of 7+3 in SWOG trials, a single-center analysis by Ravandi et al. noted a CR rate of 76% with an initial high-dose cytarabine-containing course, but reported a rate of 32% in 129 patients receiving a second similar course [6]. SWOG Cancer Network trial S1203 randomized patients with untreated AML who were 60 years of age or younger among 7+3, IA, and IA + vorinostat, thereby allowing a comparison of rates of CR and CRi after 1 and 2 cycles of induction therapy in a group of patients who met the same eligibility criteria and underwent randomization. This report analyzes data from patients randomized to the 7+3 and IA arms.The primary outcome of S1203 has been previously reported [7]. All patients had untreated AML and were \(\le\)60 years of age. Patients randomized to 7+3 (n = 261) received 100 mg/m2 cytarabine on days 1–7 by continuous infusion and 90 mg/m2 daunorubicin on days 1–3. Patients randomized to IA (n = 261) received 1500 mg/m2 cytarabine on days 1–4 by continuous infusion and 12 mg/m2 Idarubicin on days 1–3. CR and CRi were defined per contemporary consensus criteria (CR: ANC \(\ge\) 1000/mcl, platelet count \(\ge\)100,000/mcl, <5% bone marrow blasts; CRi same as CR but either ANC or platelet criteria not met). Patients who did not achieve morphologic CR or CRi after the first cycle of induction were eligible for a second cycle. Patients randomized to 7+3 were to have a marrow examination at approximately day 14 and if residual blasts were seen, reinduction was to be initiated. Patients randomized to IA were to have a bone marrow examination at approximately day 28 and if residual blasts were seen, reinduction was to be initiated. Re-induction with 7+3 called for the same dose and schedule of cytarabine with a decrease in the dose of daunorubicin to 45 mg/m2 on days 1–3; reinduction with IA was identical to induction in terms of schedule and dosing. The institutional review boards of the participating institutions approved all protocols, and patients were treated according to the Declaration of Helsinki.
期刊介绍:
Title: Leukemia
Journal Overview:
Publishes high-quality, peer-reviewed research
Covers all aspects of research and treatment of leukemia and allied diseases
Includes studies of normal hemopoiesis due to comparative relevance
Topics of Interest:
Oncogenes
Growth factors
Stem cells
Leukemia genomics
Cell cycle
Signal transduction
Molecular targets for therapy
And more
Content Types:
Original research articles
Reviews
Letters
Correspondence
Comments elaborating on significant advances and covering topical issues




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
