Nathaniel J. Myall MD , Jennifer G. Whisenant PhD , Joel W. Neal MD, PhD , Wade T. Iams MD , Karen L. Reckamp MD , Sally York MD, PhD , Lynne D. Berry PhD , Yu Shyr PhD , Leora Horn MD , Heather A. Wakelee MD , Sukhmani K. Padda MD
{"title":"Afatinib and Necitumumab in EGFR-Mutant NSCLC with Acquired Resistance to Tyrosine Kinase Inhibitors","authors":"Nathaniel J. Myall MD , Jennifer G. Whisenant PhD , Joel W. Neal MD, PhD , Wade T. Iams MD , Karen L. Reckamp MD , Sally York MD, PhD , Lynne D. Berry PhD , Yu Shyr PhD , Leora Horn MD , Heather A. Wakelee MD , Sukhmani K. Padda MD","doi":"10.1016/j.jtocrr.2024.100757","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><div>Although tyrosine kinase inhibitors (TKIs) are effective against NSCLC harboring sensitizing <em>EGFR</em> gene mutations, acquired resistance is inevitable. Preclinical studies suggest that combining EGFR TKI and monoclonal antibody therapies may have activity in <em>EGFR-</em>mutated NSCLC that has progressed on TKI therapy alone. Therefore, we prospectively evaluated afatinib plus necitumumab in patients with <em>EGFR-</em>mutated NSCLC.</div></div><div><h3>Methods</h3><div>This was a phase 1, dose-escalation, dose-expansion trial assessing the safety and efficacy of afatinib plus necitumumab. Patients had advanced or metastatic <em>EGFR-</em>mutated NSCLC with progression after (1) first-generation TKI if T790M negative, (2) subsequent line third-generation TKI if T790M positive, or (3) third-generation TKI in the first-line setting. Dose-escalation followed a 3+3 design. The primary end point of dose-expansion was objective response rate.</div></div><div><h3>Results</h3><div>A total of 22 patients with <em>EGFR</em>-mutated NSCLC were enrolled. The maximum tolerated dose was afatinib 40 mg oral daily plus necitumumab 600 mg intravenous on days 1 and 15 every 28 days. There were no grade 4 to 5 adverse events observed, and seven patients (32%) experienced grade 3 treatment-related adverse events (three rash; one each oral mucositis, diarrhea, headache, ventricular arrhythmia, and tachycardia). In the entire cohort, there were no responses observed, the median progression-free survival was 1.8 months, and the disease control rate was 36% but varied between the subgroups.</div></div><div><h3>Conclusions</h3><div>Afatinib plus necitumumab was safe but had limited activity in patients with <em>EGFR-</em>mutated NSCLC. Biomarker studies may identify patient subgroups that are more likely to benefit.</div></div>","PeriodicalId":17675,"journal":{"name":"JTO Clinical and Research Reports","volume":"6 2","pages":"Article 100757"},"PeriodicalIF":3.5000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11759541/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"JTO Clinical and Research Reports","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2666364324001279","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/11/4 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction
Although tyrosine kinase inhibitors (TKIs) are effective against NSCLC harboring sensitizing EGFR gene mutations, acquired resistance is inevitable. Preclinical studies suggest that combining EGFR TKI and monoclonal antibody therapies may have activity in EGFR-mutated NSCLC that has progressed on TKI therapy alone. Therefore, we prospectively evaluated afatinib plus necitumumab in patients with EGFR-mutated NSCLC.
Methods
This was a phase 1, dose-escalation, dose-expansion trial assessing the safety and efficacy of afatinib plus necitumumab. Patients had advanced or metastatic EGFR-mutated NSCLC with progression after (1) first-generation TKI if T790M negative, (2) subsequent line third-generation TKI if T790M positive, or (3) third-generation TKI in the first-line setting. Dose-escalation followed a 3+3 design. The primary end point of dose-expansion was objective response rate.
Results
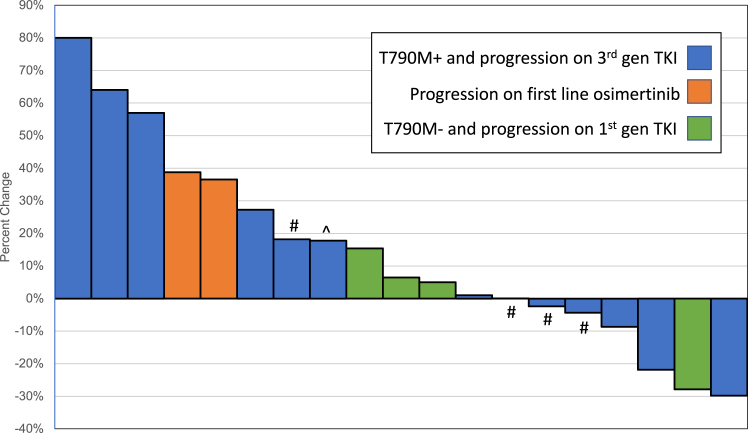
A total of 22 patients with EGFR-mutated NSCLC were enrolled. The maximum tolerated dose was afatinib 40 mg oral daily plus necitumumab 600 mg intravenous on days 1 and 15 every 28 days. There were no grade 4 to 5 adverse events observed, and seven patients (32%) experienced grade 3 treatment-related adverse events (three rash; one each oral mucositis, diarrhea, headache, ventricular arrhythmia, and tachycardia). In the entire cohort, there were no responses observed, the median progression-free survival was 1.8 months, and the disease control rate was 36% but varied between the subgroups.
Conclusions
Afatinib plus necitumumab was safe but had limited activity in patients with EGFR-mutated NSCLC. Biomarker studies may identify patient subgroups that are more likely to benefit.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
