{"title":"Diffuse Alveolar Hemorrhage Associated With Anti-PL-7 Antisynthetase Syndrome: A Case Report.","authors":"Paul Shiu, Shannon Iriza, Steven Templeton","doi":"10.1155/crpu/3715449","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Diffuse alveolar hemorrhage (DAH) is a potentially life-threatening condition which can present with hemoptysis, diffuse alveolar infiltrates, anemia, and hypoxic respiratory failure. Antisynthetase syndrome (AS) is a rare autoimmune disorder most often characterized by nonerosive arthritis, proximal muscle weakness with elevated muscle enzymes, Raynaud's phenomenon, hyperkeratosis of the digits (mechanic's hands), and interstitial lung disease. According to large population studies, AS has an annual incidence of 0.56 per 100,000 persons and prevalence of 9 per 100,000. The most common autoantibody is anti-aminoacyl-transfer RNA synthetase for histidine (anti-Jo-1) with a reported prevalence of 20%-30%, whereas anti-Pl-7 (for threonine) accounts for less than 5% of all autoimmune myositis. Specific myositis autoantibodies determine clinical phenotype. PL-7 is characterized by interstitial lung disease, myositis, and arthritis. Autoimmune myositis, specifically AS, is a rare cause of DAH. Herein, we describe the first reported case of PL-7-associated AS with DAH. <b>Case Presentation:</b> A 41-year-old female presented with worsening shortness of breath and hemoptysis. Laboratory studies included a hemoglobin of 10.5 g/dL, mildly elevated liver enzymes, and a creatine phosphokinase (CPK) of nearly 4000 U/L. CT of the chest showed diffuse ground glass opacities bilaterally. Serial aliquots of the bronchoalveolar lavage (BAL) fluid revealed progressively hemorrhagic return and histopathologic analysis consistent with DAH. Other concurrent causes of DAH were ruled out. <b>Conclusion:</b> Although rare, AS should be considered a cause of DAH, particularly in patients presenting with symptoms of muscle weakness and arthritis or with evidence of mechanic's hands.</p>","PeriodicalId":52364,"journal":{"name":"Case Reports in Pulmonology","volume":"2025 ","pages":"3715449"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11759568/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Pulmonology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crpu/3715449","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
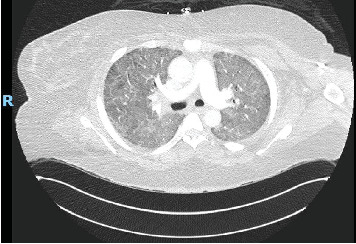
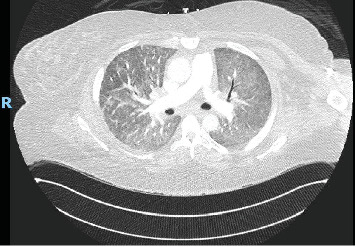
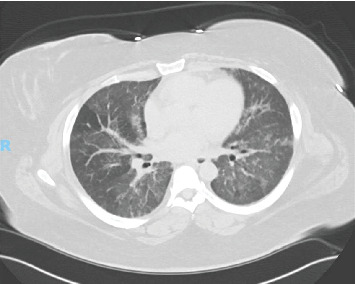
Background: Diffuse alveolar hemorrhage (DAH) is a potentially life-threatening condition which can present with hemoptysis, diffuse alveolar infiltrates, anemia, and hypoxic respiratory failure. Antisynthetase syndrome (AS) is a rare autoimmune disorder most often characterized by nonerosive arthritis, proximal muscle weakness with elevated muscle enzymes, Raynaud's phenomenon, hyperkeratosis of the digits (mechanic's hands), and interstitial lung disease. According to large population studies, AS has an annual incidence of 0.56 per 100,000 persons and prevalence of 9 per 100,000. The most common autoantibody is anti-aminoacyl-transfer RNA synthetase for histidine (anti-Jo-1) with a reported prevalence of 20%-30%, whereas anti-Pl-7 (for threonine) accounts for less than 5% of all autoimmune myositis. Specific myositis autoantibodies determine clinical phenotype. PL-7 is characterized by interstitial lung disease, myositis, and arthritis. Autoimmune myositis, specifically AS, is a rare cause of DAH. Herein, we describe the first reported case of PL-7-associated AS with DAH. Case Presentation: A 41-year-old female presented with worsening shortness of breath and hemoptysis. Laboratory studies included a hemoglobin of 10.5 g/dL, mildly elevated liver enzymes, and a creatine phosphokinase (CPK) of nearly 4000 U/L. CT of the chest showed diffuse ground glass opacities bilaterally. Serial aliquots of the bronchoalveolar lavage (BAL) fluid revealed progressively hemorrhagic return and histopathologic analysis consistent with DAH. Other concurrent causes of DAH were ruled out. Conclusion: Although rare, AS should be considered a cause of DAH, particularly in patients presenting with symptoms of muscle weakness and arthritis or with evidence of mechanic's hands.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
