{"title":"The usefulness of Charlson Comorbidity Index (CCI) scoring in predicting all-cause mortality in Outpatients with Clinical Diagnoses of COPD.","authors":"Kevin Ly, Dorothy Wakefield, Richard ZuWallack","doi":"10.1177/26335565251315876","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Since comorbid conditions are frequently present in chronic obstructive pulmonary disease (COPD) and affect outcome, a composite scoring system to quantify comorbidity might be helpful in assessing mortality risk.</p><p><strong>Methods: </strong>We tested the hypothesis that the Charlson Comorbidity Index (CCI) score at the time of an outpatient medical clinic encounter for COPD predicts all-cause mortality. Cox Proportional Hazards analyses were used in 200 randomly selected patients to relate CCI scores to all-cause mortality out to 5 years.</p><p><strong>Results: </strong>Mean age was 62 ± 10 years, 56% were female, FEV1 was 62%, CCI was 3.08 ± 2.30, and 30% had a CCI ≥ 4, indicating 3 or more comorbid conditions. All-cause mortality was 8.5% and 20% at 3 and 5 years, respectively. In univariate testing, the CCI score and hospitalizations predicted mortality, but FEV1 did not. In multivariable testing, which included covariates of age, sex, socioeconomic status, race, FEV1 percent-predicted, and all-cause hospitalizations in the preceding year, CCI expressed as a continuous variable strongly predicted mortality: hazard ratio (HR) 1.38 for each unit increase in the score (p < 0.0001). While 1 or 2 comorbid conditions were not significantly related to mortality, 3 or more comorbid conditions (compared to none) strongly predicted mortality: HR 9.80, 95% CI 3.80 to 25.00.</p><p><strong>Conclusion: </strong>Comorbidity, assessed with the CCI, is strongly predictive of mortality in outpatients with a clinical diagnosis of COPD, and this relationship appears to be non-linear. This instrument may be useful in determining prognosis in this population.</p>","PeriodicalId":73843,"journal":{"name":"Journal of multimorbidity and comorbidity","volume":"15 ","pages":"26335565251315876"},"PeriodicalIF":3.0000,"publicationDate":"2025-01-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11773518/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of multimorbidity and comorbidity","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/26335565251315876","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Since comorbid conditions are frequently present in chronic obstructive pulmonary disease (COPD) and affect outcome, a composite scoring system to quantify comorbidity might be helpful in assessing mortality risk.
Methods: We tested the hypothesis that the Charlson Comorbidity Index (CCI) score at the time of an outpatient medical clinic encounter for COPD predicts all-cause mortality. Cox Proportional Hazards analyses were used in 200 randomly selected patients to relate CCI scores to all-cause mortality out to 5 years.
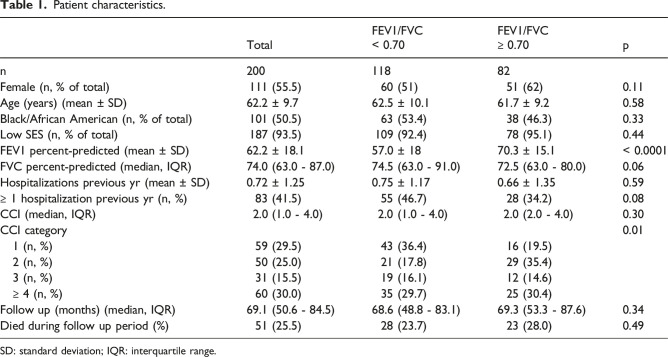
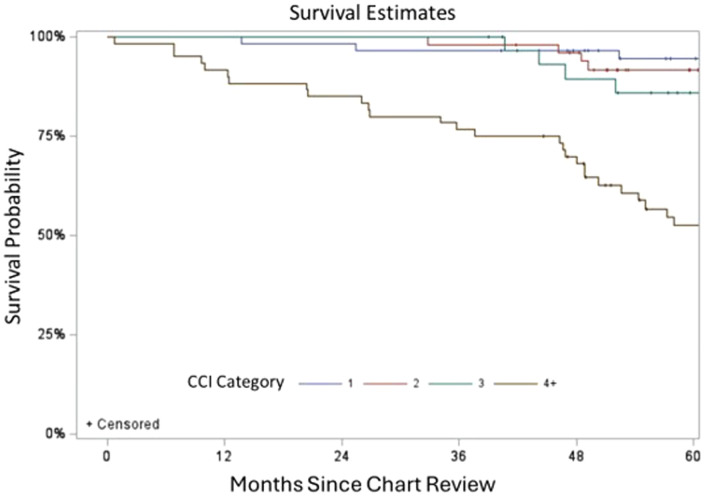
Results: Mean age was 62 ± 10 years, 56% were female, FEV1 was 62%, CCI was 3.08 ± 2.30, and 30% had a CCI ≥ 4, indicating 3 or more comorbid conditions. All-cause mortality was 8.5% and 20% at 3 and 5 years, respectively. In univariate testing, the CCI score and hospitalizations predicted mortality, but FEV1 did not. In multivariable testing, which included covariates of age, sex, socioeconomic status, race, FEV1 percent-predicted, and all-cause hospitalizations in the preceding year, CCI expressed as a continuous variable strongly predicted mortality: hazard ratio (HR) 1.38 for each unit increase in the score (p < 0.0001). While 1 or 2 comorbid conditions were not significantly related to mortality, 3 or more comorbid conditions (compared to none) strongly predicted mortality: HR 9.80, 95% CI 3.80 to 25.00.
Conclusion: Comorbidity, assessed with the CCI, is strongly predictive of mortality in outpatients with a clinical diagnosis of COPD, and this relationship appears to be non-linear. This instrument may be useful in determining prognosis in this population.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
