Ghazal Haddad, David M Maslove, Lawrence Mbuagbaw, Emilie P Belley-Côté, Bram Rochwerg
{"title":"Corticosteroids in Cardiogenic Shock: A Retrospective Analysis of the Medical Information Mart for Intensive Care-IV Database.","authors":"Ghazal Haddad, David M Maslove, Lawrence Mbuagbaw, Emilie P Belley-Côté, Bram Rochwerg","doi":"10.1097/CCE.0000000000001210","DOIUrl":null,"url":null,"abstract":"<p><strong>Importance: </strong>While corticosteroid administration in septic shock has been shown to result in faster shock reversal and lower short-term mortality, the role of corticosteroids in the management of cardiogenic shock (CS) remains unexplored.</p><p><strong>Objectives: </strong>Determine the impact of corticosteroid administration on 90-day mortality (primary outcome) in patients admitted to a critical care unit with CS.</p><p><strong>Design, setting, and participants: </strong>In this retrospective cohort study, we used the critical care database of Medical Information Mart for Intensive Care-IV, and included all adult patients diagnosed with CS excluding repeated admissions, patients with adrenal insufficiency, those receiving baseline corticosteroids, and those requiring extracorporeal life support. We considered exposure based on receiving systemic corticosteroids from 6 hours before to 24 hours post-critical care admission.</p><p><strong>Main outcomes and measures: </strong>We calculated Cox proportional hazards using multivariate analysis for 90-day mortality (primary outcome). We also explored the association of corticosteroid use with hospital length of stay, ventilator-free days (VFDs), vasopressor-free days, ventilator-associated pneumonia, central-line-associated bloodstream infections, and hyperglycemia.</p><p><strong>Results: </strong>We included 2000 eligible patients, with 143 (7.2%) receiving systemic corticosteroids. Corticosteroid-treated patients were younger (67.7 vs. 71.2 yr; p = 0.006), had higher Sequential Organ Failure Assessment scores at baseline (9.4 vs. 7.8; p < 0.001), and more often required vasopressors (78% vs. 63%; p < 0.001), and invasive mechanical ventilation (73% vs. 45%; p < 0.001). Corticosteroid use was associated with increased 90-day mortality in multivariate analysis (hazard ratio, 1.60; 95% CI, 1.25-2.05) and fewer VFDs (2.8 d fewer; 95% CI, 0.35-5.26) with no effect on other secondary outcomes.</p><p><strong>Conclusions and relevance: </strong>Use of corticosteroids may be associated with increased mortality and a reduction in VFDs in patients admitted to critical care with CS. These findings suggesting potential harm of corticosteroids in CS might reflect unmeasured confounding and require corroboration through additional observational studies and ultimately randomized clinical trials.</p>","PeriodicalId":93957,"journal":{"name":"Critical care explorations","volume":"7 2","pages":"e1210"},"PeriodicalIF":2.7000,"publicationDate":"2025-01-31","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11789865/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Critical care explorations","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1097/CCE.0000000000001210","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Importance: While corticosteroid administration in septic shock has been shown to result in faster shock reversal and lower short-term mortality, the role of corticosteroids in the management of cardiogenic shock (CS) remains unexplored.
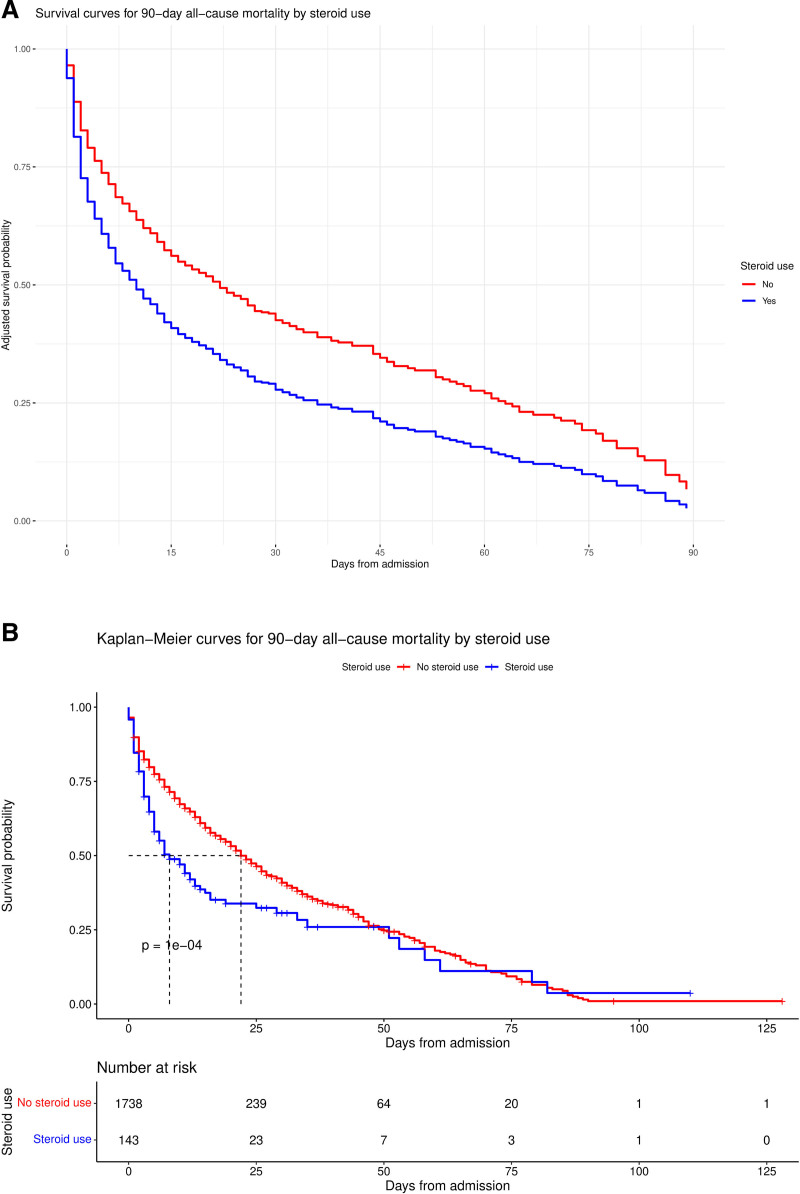
Objectives: Determine the impact of corticosteroid administration on 90-day mortality (primary outcome) in patients admitted to a critical care unit with CS.
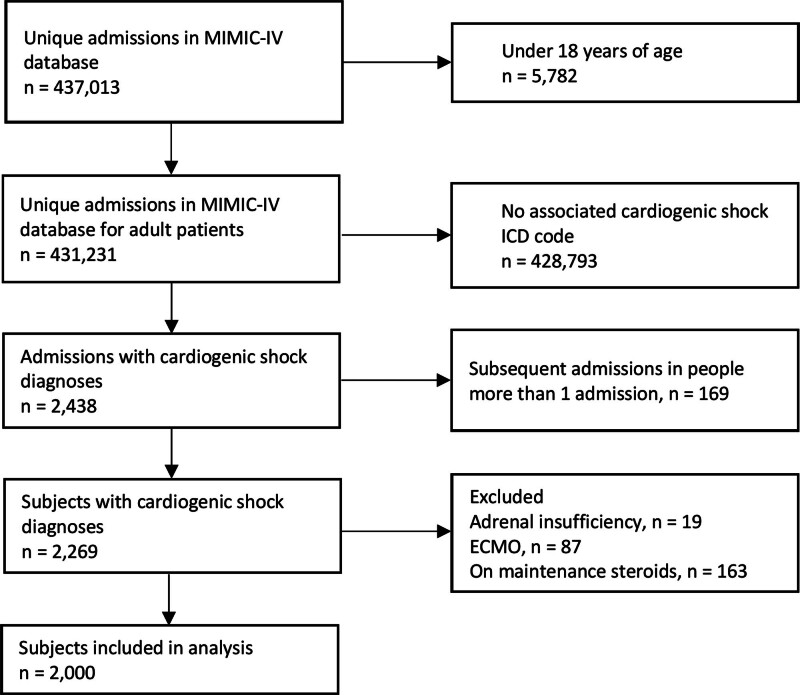
Design, setting, and participants: In this retrospective cohort study, we used the critical care database of Medical Information Mart for Intensive Care-IV, and included all adult patients diagnosed with CS excluding repeated admissions, patients with adrenal insufficiency, those receiving baseline corticosteroids, and those requiring extracorporeal life support. We considered exposure based on receiving systemic corticosteroids from 6 hours before to 24 hours post-critical care admission.
Main outcomes and measures: We calculated Cox proportional hazards using multivariate analysis for 90-day mortality (primary outcome). We also explored the association of corticosteroid use with hospital length of stay, ventilator-free days (VFDs), vasopressor-free days, ventilator-associated pneumonia, central-line-associated bloodstream infections, and hyperglycemia.
Results: We included 2000 eligible patients, with 143 (7.2%) receiving systemic corticosteroids. Corticosteroid-treated patients were younger (67.7 vs. 71.2 yr; p = 0.006), had higher Sequential Organ Failure Assessment scores at baseline (9.4 vs. 7.8; p < 0.001), and more often required vasopressors (78% vs. 63%; p < 0.001), and invasive mechanical ventilation (73% vs. 45%; p < 0.001). Corticosteroid use was associated with increased 90-day mortality in multivariate analysis (hazard ratio, 1.60; 95% CI, 1.25-2.05) and fewer VFDs (2.8 d fewer; 95% CI, 0.35-5.26) with no effect on other secondary outcomes.
Conclusions and relevance: Use of corticosteroids may be associated with increased mortality and a reduction in VFDs in patients admitted to critical care with CS. These findings suggesting potential harm of corticosteroids in CS might reflect unmeasured confounding and require corroboration through additional observational studies and ultimately randomized clinical trials.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
