Beatrice A. Brumley MD , Run Yu MD, PhD , Shadfar Bahri MD , Jane Rhyu MD
{"title":"Malignant Paraganglioma With Calvarial Metastases Presenting With Recurrent Catecholamine-Induced Cardiomyopathy","authors":"Beatrice A. Brumley MD , Run Yu MD, PhD , Shadfar Bahri MD , Jane Rhyu MD","doi":"10.1016/j.aace.2024.09.006","DOIUrl":null,"url":null,"abstract":"<div><h3>Background/Objective</h3><div>Cranial metastases rarely occur in malignant paragangliomas (PGLs) or pheochromocytomas, which usually metastasize to the liver, bone, lungs, and lymph nodes. Early detection and intervention with a multidisciplinary approach are crucial given the critical location.</div></div><div><h3>Case Report</h3><div>Our patient was a 31-year-old man diagnosed with periaortic PGL and succinate dehydrogenase subunit B pathogenic variant at the age of 9 years with cardiac arrest. He developed intra-abdominal and skeletal metastatic disease by the age of 14 years and treated with surgery, chemotherapy, and radiation. After being lost to follow-up, the patient presented emergently with headache, palpitations, hypertensive crisis, type 2 non-ST-elevation myocardial infarction, and catecholamine-induced cardiomyopathy, with plasma free metanephrine level of 61.0 pg/mL (0.0-88.0 pg/mL) and elevated serum free normetanephrine level of 662.9 pg/mL (0.0-210.1 pg/mL). Imaging showed a right frontal calvarial lesion, with 4.9-cm intracranial dural and 4.9-cm extracranial components, and a 1.5-cm occipital bone lesion. Following adrenergic blockade, the patient underwent resection of the frontal lesion with pathology showing metastatic PGL.</div></div><div><h3>Discussion</h3><div>A multidisciplinary team was consulted. Because of potential neurotoxicity, radiology advised against radiotherapy. Oncology advised monitoring. Seven months postoperatively, gallium-68 dodecane tetraacetic acid–octreotate positron emission tomography/computed tomography showed no recurrence at the surgical site, stable occipital lesion, and additional skeletal metastases. The patient is planned for peptide receptor radionuclide therapy.</div></div><div><h3>Conclusion</h3><div>Our case highlights the importance of active surveillance in PGL and pheochromocytoma to allow early intervention for metastatic disease and reviews the controversial management of rare calvarial or cerebral metastases, including peptide receptor radionuclide therapy.</div></div>","PeriodicalId":7051,"journal":{"name":"AACE Clinical Case Reports","volume":"11 1","pages":"Pages 24-28"},"PeriodicalIF":1.2000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11784624/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"AACE Clinical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S237606052400107X","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"Medicine","Score":null,"Total":0}
引用次数: 0
Abstract
Background/Objective
Cranial metastases rarely occur in malignant paragangliomas (PGLs) or pheochromocytomas, which usually metastasize to the liver, bone, lungs, and lymph nodes. Early detection and intervention with a multidisciplinary approach are crucial given the critical location.
Case Report
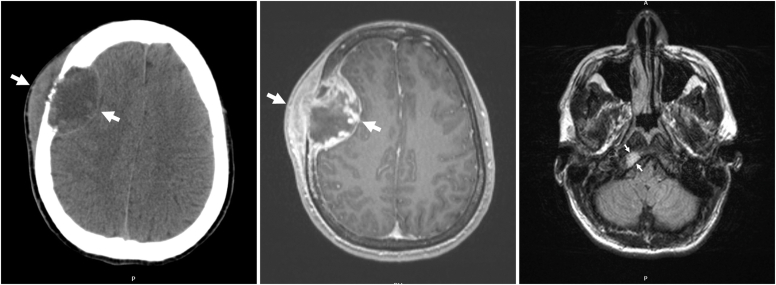
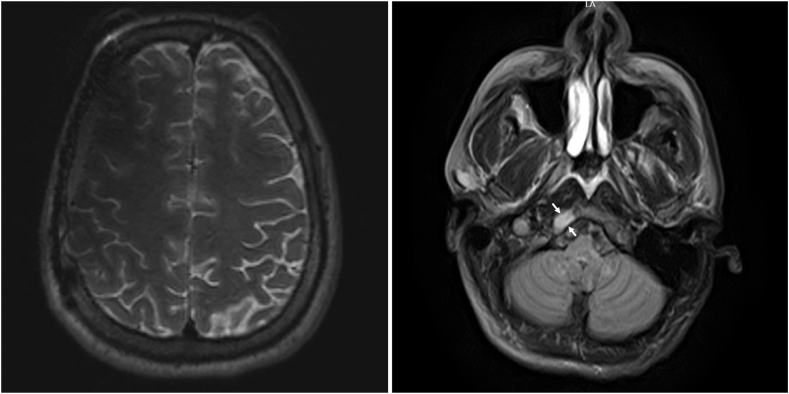
Our patient was a 31-year-old man diagnosed with periaortic PGL and succinate dehydrogenase subunit B pathogenic variant at the age of 9 years with cardiac arrest. He developed intra-abdominal and skeletal metastatic disease by the age of 14 years and treated with surgery, chemotherapy, and radiation. After being lost to follow-up, the patient presented emergently with headache, palpitations, hypertensive crisis, type 2 non-ST-elevation myocardial infarction, and catecholamine-induced cardiomyopathy, with plasma free metanephrine level of 61.0 pg/mL (0.0-88.0 pg/mL) and elevated serum free normetanephrine level of 662.9 pg/mL (0.0-210.1 pg/mL). Imaging showed a right frontal calvarial lesion, with 4.9-cm intracranial dural and 4.9-cm extracranial components, and a 1.5-cm occipital bone lesion. Following adrenergic blockade, the patient underwent resection of the frontal lesion with pathology showing metastatic PGL.
Discussion
A multidisciplinary team was consulted. Because of potential neurotoxicity, radiology advised against radiotherapy. Oncology advised monitoring. Seven months postoperatively, gallium-68 dodecane tetraacetic acid–octreotate positron emission tomography/computed tomography showed no recurrence at the surgical site, stable occipital lesion, and additional skeletal metastases. The patient is planned for peptide receptor radionuclide therapy.
Conclusion
Our case highlights the importance of active surveillance in PGL and pheochromocytoma to allow early intervention for metastatic disease and reviews the controversial management of rare calvarial or cerebral metastases, including peptide receptor radionuclide therapy.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
