Propensity score-matched real-world comparative treatment outcomes of Janus kinase inhibitors for ulcerative colitis in patients with and without prior exposure to anti-tumor necrosis factor α antibody.
{"title":"Propensity score-matched real-world comparative treatment outcomes of Janus kinase inhibitors for ulcerative colitis in patients with and without prior exposure to anti-tumor necrosis factor α antibody.","authors":"Maiko Ikenouchi, Hirokazu Fukui, Soichi Yagi, Akira Nogami, Koji Kaku, Toshiyuki Sato, Mikio Kawai, Koji Kamikozuru, Yoko Yokoyama, Tetsuya Takagawa, Toshihiko Tomita, Taku Kobayashi, Shinichiro Shinzaki","doi":"10.5217/ir.2024.00148","DOIUrl":null,"url":null,"abstract":"<p><strong>Background/aims: </strong>Tofacitinib (TFB), filgotinib (FIL), and upadacitinib (UPA) are Janus kinase (JAK) inhibitors approved for moderate-to-severe ulcerative colitis (UC). The appropriate positioning of each JAK inhibitor in the treatment algorithm, however, is unclear. Furthermore, real-world efficacy of JAK inhibitors for patients with UC and prior anti-tumor necrosis factor α antibody (aTNF) treatment are not fully investigated. We compared the efficacy and safety of 3 JAK inhibitors in patients with UC, considering their prior aTNF exposure.</p><p><strong>Methods: </strong>A retrospective study was conducted in patients with UC who started TFB, FIL, or UPA at 2 academic centers. This propensity score-matched cohort study assessed the effectiveness of the 3 JAK inhibitors for UC in patients with and without prior aTNF exposure, comparing steroid-free clinical remission and response rates after 8 weeks.</p><p><strong>Results: </strong>Among 274 patients who met the inclusion criteria, 145 experienced aTNF exposure (TFB: 59.2%, 100/169; FIL: 34.5%, 20/58; UPA: 53.2%, 25/47). Based on propensity score-matching, UPA led to a higher steroid-free clinical remission rates than TFB (adjusted odds ratio [aOR], 5.57; 95% confidence interval [CI], 1.42-21.90) or FIL (aOR, 9.00; 95% CI, 1.42-57.10) in patients exposed to aTNF. Steroid-free clinical remission and clinical response rates did not differ significantly between each group in patients non-exposed to aTNF. The incidence of adverse events was slightly higher with UPA than TFB or FIL.</p><p><strong>Conclusions: </strong>UPA may be more effective for UC than TFB or FIL, especially in patients with previous aTNF exposure, although consideration should be given to adverse events.</p>","PeriodicalId":14481,"journal":{"name":"Intestinal Research","volume":" ","pages":"464-474"},"PeriodicalIF":3.9000,"publicationDate":"2025-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12590076/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intestinal Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5217/ir.2024.00148","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/3 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background/aims: Tofacitinib (TFB), filgotinib (FIL), and upadacitinib (UPA) are Janus kinase (JAK) inhibitors approved for moderate-to-severe ulcerative colitis (UC). The appropriate positioning of each JAK inhibitor in the treatment algorithm, however, is unclear. Furthermore, real-world efficacy of JAK inhibitors for patients with UC and prior anti-tumor necrosis factor α antibody (aTNF) treatment are not fully investigated. We compared the efficacy and safety of 3 JAK inhibitors in patients with UC, considering their prior aTNF exposure.
Methods: A retrospective study was conducted in patients with UC who started TFB, FIL, or UPA at 2 academic centers. This propensity score-matched cohort study assessed the effectiveness of the 3 JAK inhibitors for UC in patients with and without prior aTNF exposure, comparing steroid-free clinical remission and response rates after 8 weeks.
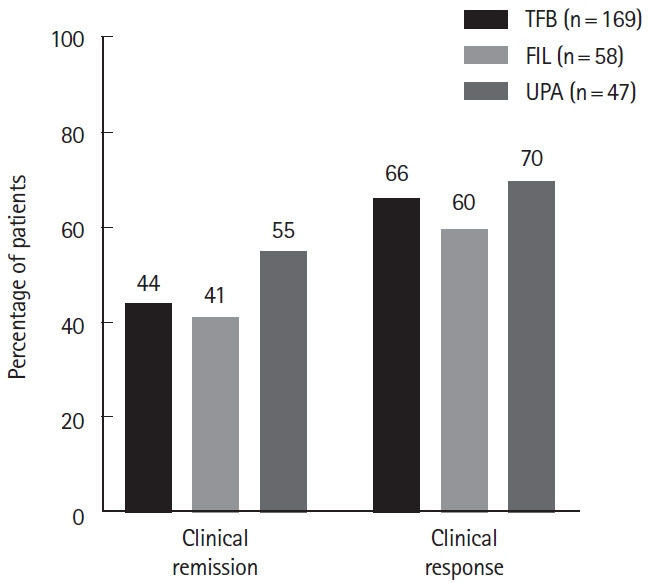
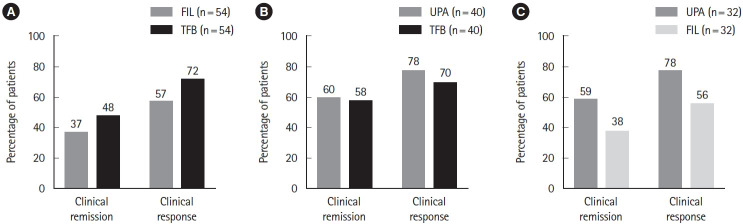
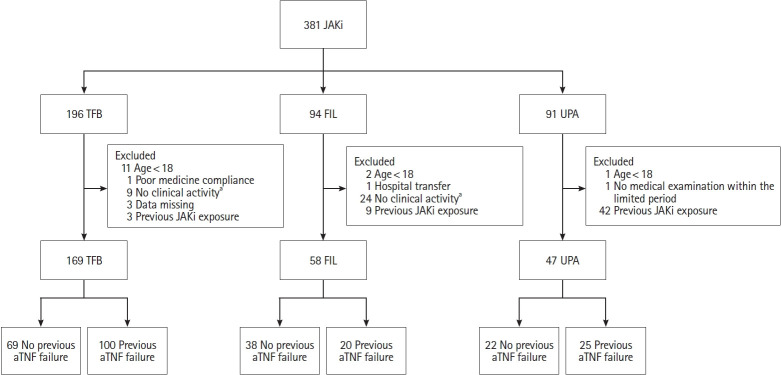
Results: Among 274 patients who met the inclusion criteria, 145 experienced aTNF exposure (TFB: 59.2%, 100/169; FIL: 34.5%, 20/58; UPA: 53.2%, 25/47). Based on propensity score-matching, UPA led to a higher steroid-free clinical remission rates than TFB (adjusted odds ratio [aOR], 5.57; 95% confidence interval [CI], 1.42-21.90) or FIL (aOR, 9.00; 95% CI, 1.42-57.10) in patients exposed to aTNF. Steroid-free clinical remission and clinical response rates did not differ significantly between each group in patients non-exposed to aTNF. The incidence of adverse events was slightly higher with UPA than TFB or FIL.
Conclusions: UPA may be more effective for UC than TFB or FIL, especially in patients with previous aTNF exposure, although consideration should be given to adverse events.
期刊介绍:
Intestinal Research (Intest Res) is the joint official publication of the Asian Organization for Crohn''s and Colitis (AOCC), Chinese Society of IBD (CSIBD), Japanese Society for IBD (JSIBD), Korean Association for the Study of Intestinal Diseases (KASID), Taiwan Society of IBD (TSIBD) and Colitis Crohn''s Foundation (India) (CCF, india). The aim of the Journal is to provide broad and in-depth analysis of intestinal diseases, especially inflammatory bowel disease, which shows increasing tendency and significance. As a Journal specialized in clinical and translational research in gastroenterology, it encompasses multiple aspects of diseases originated from the small and large intestines. The Journal also seeks to propagate and exchange useful innovations, both in ideas and in practice, within the research community. As a mode of scholarly communication, it encourages scientific investigation through the rigorous peer-review system and constitutes a qualified and continual platform for sharing studies of researchers and practitioners. Specifically, the Journal presents up-to-date coverage of medical researches on the physiology, epidemiology, pathophysiology, clinical presentations, and therapeutic interventions of the intestinal diseases. General topics of interest include inflammatory bowel disease, colon and small intestine cancer or polyp, endoscopy, irritable bowel syndrome and other motility disorders, infectious enterocolitis, intestinal tuberculosis, and so forth. The Journal publishes diverse types of academic materials such as editorials, clinical and basic reviews, original articles, case reports, letters to the editor, brief communications, perspective, statement or commentary, and images that are useful to clinicians and researchers.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
