Lukas Sturm , Michael Schultheiss , Fabian Stöhr , Christian Labenz , Benjamin Maasoumy , Anja Tiede , Michael Praktiknjo , Leon Louis Seifert , Timo Alexander Auer , Uli Fehrenbach , Felix Piecha , Aenne Harberts , Johannes Kluwe , Tony Bruns , Maike Rebecca Pollmanns , Johannes Chang , Jakub Grobelski , Christian Jansen , Carsten Meyer , Marlene Reincke , Dominik Bettinger
{"title":"Freiburg index of post-TIPS survival (FIPS) identifies patients at risk of further decompensation and ACLF after TIPS","authors":"Lukas Sturm , Michael Schultheiss , Fabian Stöhr , Christian Labenz , Benjamin Maasoumy , Anja Tiede , Michael Praktiknjo , Leon Louis Seifert , Timo Alexander Auer , Uli Fehrenbach , Felix Piecha , Aenne Harberts , Johannes Kluwe , Tony Bruns , Maike Rebecca Pollmanns , Johannes Chang , Jakub Grobelski , Christian Jansen , Carsten Meyer , Marlene Reincke , Dominik Bettinger","doi":"10.1016/j.jhep.2025.01.030","DOIUrl":null,"url":null,"abstract":"<div><h3>Background & Aims</h3><div>The Freiburg index of post-TIPS survival (FIPS) defines a high-risk group of patients with significantly reduced survival following transjugular intrahepatic portosystemic shunt (TIPS) implantation. However, the clinical hallmarks responsible for these patients’ unfavorable outcome remain to be identified. Therefore, the present study aimed to characterize the clinical course after TIPS implantation according to the FIPS.</div></div><div><h3>Methods</h3><div>A total of 1,359 patients with cirrhosis allocated to TIPS implantation for treatment of recurrent or refractory ascites or secondary prophylaxis of variceal bleeding from eight tertiary centers were retrospectively included. The patients’ clinical course following TIPS placement was analyzed, stratified according to the FIPS. The primary study outcome was further decompensation within 90 days after TIPS; secondary outcomes were acute-on-chronic liver failure (ACLF) within 90 days and 1-year transplant-free survival.</div></div><div><h3>Results</h3><div>Further decompensation after TIPS implantation was significantly more frequent in FIPS high-risk patients compared to low-risk patients (cumulative incidence function 0.58 <em>vs.</em> 0.38, <em>p <</em>0.001). Moreover, FIPS high-risk patients developed ACLF significantly more often (0.18 <em>vs.</em> 0.08; <em>p =</em> 0.008). Uni- and multivariable competing risk regression analyses confirmed that high-risk FIPS independently predicted further decompensation (subdistribution hazard ratio 1.974; 95% CI 1.531–2.544; <em>p <</em>0.001) and ACLF (subdistribution hazard ratio 2.586; 95% CI 1.449–4.616; <em>p =</em> 0.001) after TIPS. Importantly, further decompensation and ACLF after TIPS were associated with significantly reduced transplant-free survival.</div></div><div><h3>Conclusions</h3><div>The present study reveals that the FIPS predicts development of further decompensation and ACLF after TIPS implantation. These events are responsible for impaired transplant-free survival in FIPS high-risk patients. These results pave the way for the development of tailored clinical management strategies.</div></div><div><h3>Impact and implications</h3><div>Prognostication after transjugular intrahepatic portosystemic shunt (TIPS) implantation is challenging. Several clinical scores have been proposed in this context, such as the Freiburg index of post-TIPS survival (FIPS). The FIPS can identify a high-risk group of patients with significantly reduced survival after TIPS. However, to understand the reasons for these patients’ unfavorable outcome, their clinical course after TIPS needs to be characterized. This study reveals that the FIPS predicts development of further decompensation and acute-on-chronic liver failure after TIPS implantation, which are responsible for the poor prognosis of FIPS high-risk patients. Therefore, the present results may be useful for tailored decision making in patients allocated to TIPS implantation.</div></div>","PeriodicalId":15888,"journal":{"name":"Journal of Hepatology","volume":"83 2","pages":"Pages 348-357"},"PeriodicalIF":33.0000,"publicationDate":"2025-08-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Hepatology","FirstCategoryId":"3","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S0168827825000674","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/4 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background & Aims
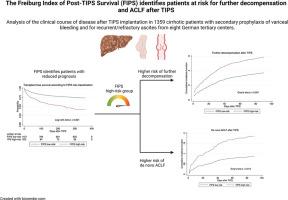
The Freiburg index of post-TIPS survival (FIPS) defines a high-risk group of patients with significantly reduced survival following transjugular intrahepatic portosystemic shunt (TIPS) implantation. However, the clinical hallmarks responsible for these patients’ unfavorable outcome remain to be identified. Therefore, the present study aimed to characterize the clinical course after TIPS implantation according to the FIPS.
Methods
A total of 1,359 patients with cirrhosis allocated to TIPS implantation for treatment of recurrent or refractory ascites or secondary prophylaxis of variceal bleeding from eight tertiary centers were retrospectively included. The patients’ clinical course following TIPS placement was analyzed, stratified according to the FIPS. The primary study outcome was further decompensation within 90 days after TIPS; secondary outcomes were acute-on-chronic liver failure (ACLF) within 90 days and 1-year transplant-free survival.
Results
Further decompensation after TIPS implantation was significantly more frequent in FIPS high-risk patients compared to low-risk patients (cumulative incidence function 0.58 vs. 0.38, p <0.001). Moreover, FIPS high-risk patients developed ACLF significantly more often (0.18 vs. 0.08; p = 0.008). Uni- and multivariable competing risk regression analyses confirmed that high-risk FIPS independently predicted further decompensation (subdistribution hazard ratio 1.974; 95% CI 1.531–2.544; p <0.001) and ACLF (subdistribution hazard ratio 2.586; 95% CI 1.449–4.616; p = 0.001) after TIPS. Importantly, further decompensation and ACLF after TIPS were associated with significantly reduced transplant-free survival.
Conclusions
The present study reveals that the FIPS predicts development of further decompensation and ACLF after TIPS implantation. These events are responsible for impaired transplant-free survival in FIPS high-risk patients. These results pave the way for the development of tailored clinical management strategies.
Impact and implications
Prognostication after transjugular intrahepatic portosystemic shunt (TIPS) implantation is challenging. Several clinical scores have been proposed in this context, such as the Freiburg index of post-TIPS survival (FIPS). The FIPS can identify a high-risk group of patients with significantly reduced survival after TIPS. However, to understand the reasons for these patients’ unfavorable outcome, their clinical course after TIPS needs to be characterized. This study reveals that the FIPS predicts development of further decompensation and acute-on-chronic liver failure after TIPS implantation, which are responsible for the poor prognosis of FIPS high-risk patients. Therefore, the present results may be useful for tailored decision making in patients allocated to TIPS implantation.
背景,目的:TIPS术后生存的Freiburg指数(FIPS)定义了经颈静脉肝内门静脉系统分流术(TIPS)植入术后生存率显著降低的高危患者群体。然而,导致这些患者不良结果的临床标志仍有待确定。因此,本研究旨在根据FIPS来描述TIPS植入后的临床过程。方法回顾性分析来自8个三级中心的1359例肝硬化患者进行TIPS植入术治疗复发性或难治性腹水或静脉曲张出血的二级预防。分析患者置放TIPS后的临床病程,根据FIPS进行分层。主要研究结果是TIPS后90天内肝硬化进一步失代偿,次要结果是90天内急性慢性肝功能衰竭(ACLF)和1年无移植生存期。结果与低危患者相比,FIPS高危患者在TIPS植入后出现进一步失代偿的频率更高(累积发生率函数0.58 vs 0.38, p <;0.001)。此外,FIPS高危患者发生ACLF的频率显著高于其他高危患者(0.18 vs. 0.08;P = 0.008)。单变量和多变量竞争风险回归分析证实,FIPS高危组独立预测进一步失代偿(sHR 1.974, 95% CI 1.531 - 2.544, p <;0.001)和TIPS后ACLF (sHR 2.586, 95% CI 1.449 - 4.616, p = 0.001)。重要的是,TIPS后进一步失代偿和ACLF与显著降低的无移植生存相关。结论FIPS可预测TIPS植入后进一步失代偿和ACLF的发展。这些事件是FIPS高危患者无移植生存受损的原因。这些结果为量身定制的临床管理策略的发展铺平了道路。
期刊介绍:
The Journal of Hepatology is the official publication of the European Association for the Study of the Liver (EASL). It is dedicated to presenting clinical and basic research in the field of hepatology through original papers, reviews, case reports, and letters to the Editor. The Journal is published in English and may consider supplements that pass an editorial review.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
