{"title":"Management of mycosis fungoides and Sézary syndrome with mogamulizumab in combination with psoralen plus UVA: two case reports.","authors":"Andrea Bernardelli, Carlo Visco","doi":"10.1177/20406207251317165","DOIUrl":null,"url":null,"abstract":"<p><p>This report describes the cases of two patients with mycosis fungoides and Sézary syndrome (MF/SS) who achieved clinical benefit with mogamulizumab combination therapies. Case 1 is a 56-year-old male with stage IIIB (T4NxM0B1) MF, which later progressed into SS, with ongoing skin symptoms (erythema, lichenified skin, and pruritis) and axillary and inguinal lymphadenomegaly. Skin-directed and systemic therapies failed to achieve a long-lasting response in this patient. Mogamulizumab (1 mg/kg once weekly for 4 weeks; once every 2 weeks thereafter) yielded temporary improvement in skin symptoms, but progression in the skin was confirmed after ~2 months. Subsequently, the combination of mogamulizumab with psoralen plus ultraviolet light A (PUVA) yielded a partial response; however, PUVA was discontinued due to phototoxicity and mogamulizumab was continued as monotherapy. At the latest evaluation, clinical improvement in the skin and reduced lymphadenomegaly were evident with ongoing mogamulizumab monotherapy; the patient is awaiting allogeneic hematopoietic stem cell transplantation. Case 2 is an 80-year-old male with stage IIIB (T4NxM0B1) granulomatous variant MF who presented with diffuse erythema with desquamation, ectropion, and inguinal lymphadenopathy. Treatment with oral prednisone and bexarotene failed to achieve adequate, long-lasting responses. Mogamulizumab (1 mg/kg once weekly for 4 weeks; once every 2 weeks thereafter) monotherapy yielded an initial improvement, characterized by less intense erythema, but the improvement was not sustained. Mogamulizumab was supplemented with oral prednisone and then PUVA; this combination resulted in improvement in the skin. PUVA was stopped due to unavailability, and methotrexate (10 mg once weekly) was initiated alongside continued mogamulizumab; this led to improvement in erythema. The patient continued mogamulizumab plus methotrexate with improving clinical status, prior to their death, which was deemed to be unlikely to be related to treatment. Our experience suggests that, in principle, mogamulizumab can be used in combination with other therapies; however, further research is needed.</p>","PeriodicalId":23048,"journal":{"name":"Therapeutic Advances in Hematology","volume":"16 ","pages":"20406207251317165"},"PeriodicalIF":3.1000,"publicationDate":"2025-02-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11792013/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Hematology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20406207251317165","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"HEMATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
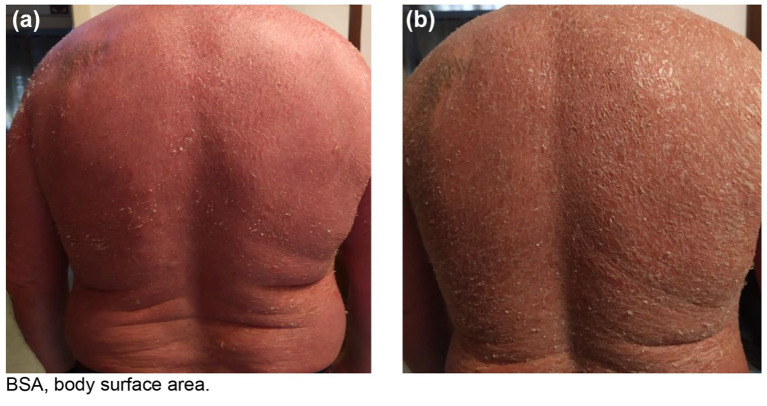
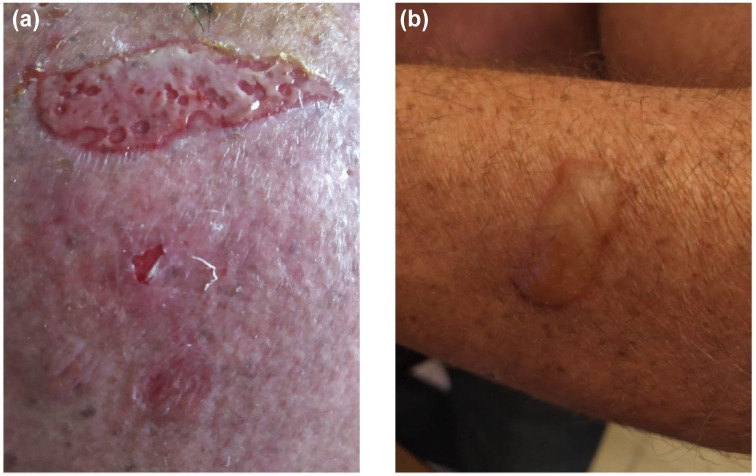
This report describes the cases of two patients with mycosis fungoides and Sézary syndrome (MF/SS) who achieved clinical benefit with mogamulizumab combination therapies. Case 1 is a 56-year-old male with stage IIIB (T4NxM0B1) MF, which later progressed into SS, with ongoing skin symptoms (erythema, lichenified skin, and pruritis) and axillary and inguinal lymphadenomegaly. Skin-directed and systemic therapies failed to achieve a long-lasting response in this patient. Mogamulizumab (1 mg/kg once weekly for 4 weeks; once every 2 weeks thereafter) yielded temporary improvement in skin symptoms, but progression in the skin was confirmed after ~2 months. Subsequently, the combination of mogamulizumab with psoralen plus ultraviolet light A (PUVA) yielded a partial response; however, PUVA was discontinued due to phototoxicity and mogamulizumab was continued as monotherapy. At the latest evaluation, clinical improvement in the skin and reduced lymphadenomegaly were evident with ongoing mogamulizumab monotherapy; the patient is awaiting allogeneic hematopoietic stem cell transplantation. Case 2 is an 80-year-old male with stage IIIB (T4NxM0B1) granulomatous variant MF who presented with diffuse erythema with desquamation, ectropion, and inguinal lymphadenopathy. Treatment with oral prednisone and bexarotene failed to achieve adequate, long-lasting responses. Mogamulizumab (1 mg/kg once weekly for 4 weeks; once every 2 weeks thereafter) monotherapy yielded an initial improvement, characterized by less intense erythema, but the improvement was not sustained. Mogamulizumab was supplemented with oral prednisone and then PUVA; this combination resulted in improvement in the skin. PUVA was stopped due to unavailability, and methotrexate (10 mg once weekly) was initiated alongside continued mogamulizumab; this led to improvement in erythema. The patient continued mogamulizumab plus methotrexate with improving clinical status, prior to their death, which was deemed to be unlikely to be related to treatment. Our experience suggests that, in principle, mogamulizumab can be used in combination with other therapies; however, further research is needed.
期刊介绍:
Therapeutic Advances in Hematology delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies across all areas of hematology. The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in hematology, providing a forum in print and online for publishing the highest quality articles in this area.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
