Karol M Pencina, A Michael Lincoff, Eric A Klein, Steven E Nissen, Yili Valentine Shang, Nader Khan, Xue Li, Anna Chan, Michael G Miller, Shalender Bhasin
{"title":"Testosterone Replacement Therapy and Risk of COVID-19 and Effect of COVID-19 on Testosterone's Treatment Effect.","authors":"Karol M Pencina, A Michael Lincoff, Eric A Klein, Steven E Nissen, Yili Valentine Shang, Nader Khan, Xue Li, Anna Chan, Michael G Miller, Shalender Bhasin","doi":"10.1210/jendso/bvaf002","DOIUrl":null,"url":null,"abstract":"<p><strong>Context: </strong>Whether circulating testosterone, dihydrotestosterone, and estradiol levels or testosterone replacement therapy (TRT) affects the risk of COVID-19 and whether COVID-19 affects response to TRT remains unknown.</p><p><strong>Objective: </strong>The study evaluated whether baseline testosterone, dihydrotestosterone, and estradiol levels or TRT are associated with risk of developing COVID-19 and whether COVID-19 affects treatment response to TRT.</p><p><strong>Methods: </strong>Among 5204 men, aged 45 to 80 years, with hypogonadism in the TRAVERSE trial, 379 developed COVID-19. We compared baseline and on-treatment hormone levels, and safety and efficacy in participants with and without COVID-19 diagnosis.</p><p><strong>Results: </strong>Neither baseline nor on-treatment testosterone, estradiol, and dihydrotestosterone levels prior to COVID-19 differed significantly between men with and without COVID-19 diagnosis. Incidence of COVID-19 was similar in participants randomized to TRT or placebo groups (3-year Kaplan-Meier incidence 8.0% in TRT and 8.6% in placebo group, <i>P</i> = .823). Incidences of COVID-19-related hospitalizations (38.5% vs 32.8%, <i>P</i> = .222) and deaths (12.8% vs 8.9%, <i>P</i> = .247) were similar in the TRT and placebo groups. Changes in hypogonadal symptoms, libido, energy, and hemoglobin/hematocrit in response to TRT were attenuated in testosterone-treated men who developed COVID-19. Incidences of major adverse cardiovascular events, venous thromboembolism, and acute kidney injury were similar in those with COVID-19 diagnosis and those without.</p><p><strong>Conclusion: </strong>In men with hypogonadism and cardiovascular disease (CVD) or increased risk of CVD, baseline and pre-COVID-19 on-treatment testosterone, dihydrotestosterone, and estradiol levels were similar in those who developed COVID-19 and those who did not. TRT did not affect the risk of COVID-19. COVID-19 attenuated the treatment response to TRT.</p>","PeriodicalId":17334,"journal":{"name":"Journal of the Endocrine Society","volume":"9 3","pages":"bvaf002"},"PeriodicalIF":3.1000,"publicationDate":"2025-02-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11795193/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of the Endocrine Society","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1210/jendso/bvaf002","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/4 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Context: Whether circulating testosterone, dihydrotestosterone, and estradiol levels or testosterone replacement therapy (TRT) affects the risk of COVID-19 and whether COVID-19 affects response to TRT remains unknown.
Objective: The study evaluated whether baseline testosterone, dihydrotestosterone, and estradiol levels or TRT are associated with risk of developing COVID-19 and whether COVID-19 affects treatment response to TRT.
Methods: Among 5204 men, aged 45 to 80 years, with hypogonadism in the TRAVERSE trial, 379 developed COVID-19. We compared baseline and on-treatment hormone levels, and safety and efficacy in participants with and without COVID-19 diagnosis.
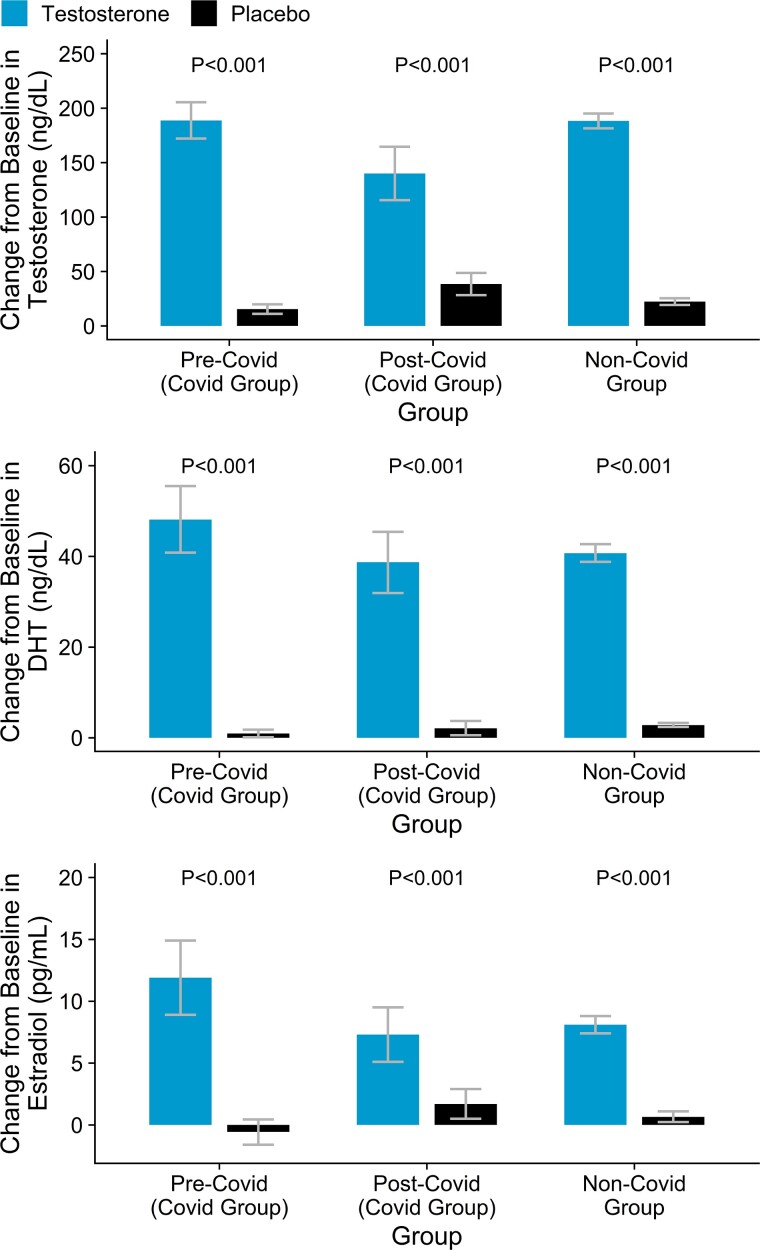
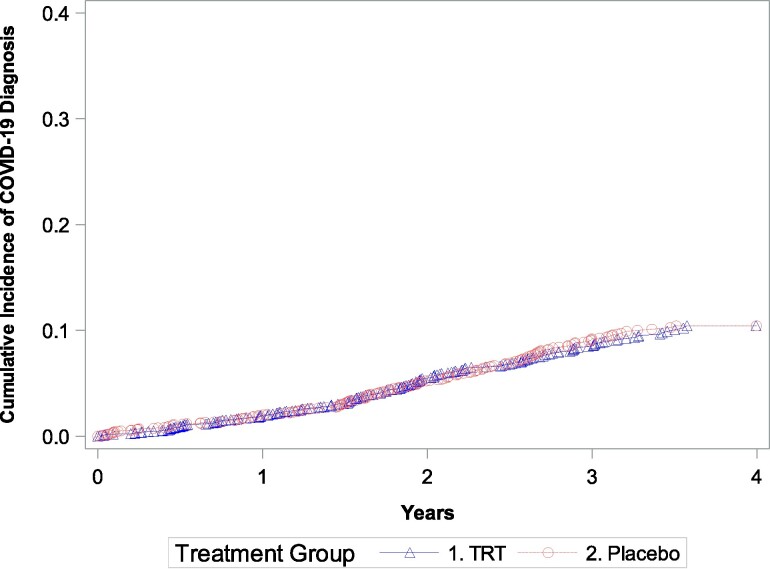
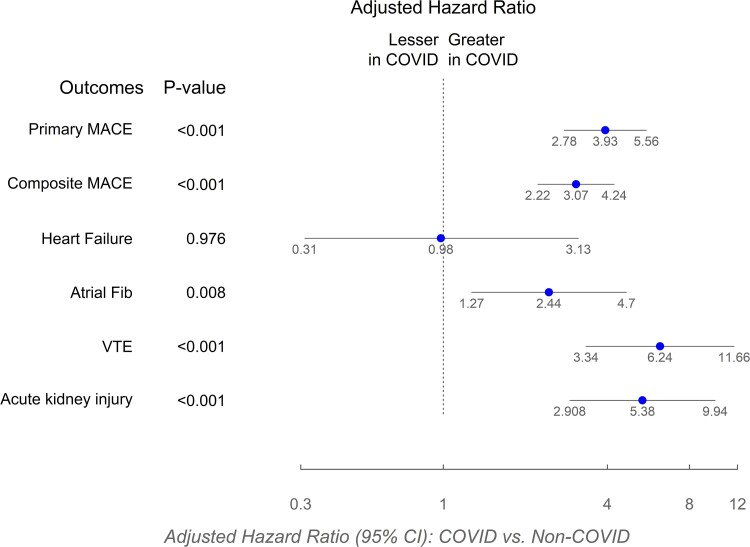
Results: Neither baseline nor on-treatment testosterone, estradiol, and dihydrotestosterone levels prior to COVID-19 differed significantly between men with and without COVID-19 diagnosis. Incidence of COVID-19 was similar in participants randomized to TRT or placebo groups (3-year Kaplan-Meier incidence 8.0% in TRT and 8.6% in placebo group, P = .823). Incidences of COVID-19-related hospitalizations (38.5% vs 32.8%, P = .222) and deaths (12.8% vs 8.9%, P = .247) were similar in the TRT and placebo groups. Changes in hypogonadal symptoms, libido, energy, and hemoglobin/hematocrit in response to TRT were attenuated in testosterone-treated men who developed COVID-19. Incidences of major adverse cardiovascular events, venous thromboembolism, and acute kidney injury were similar in those with COVID-19 diagnosis and those without.
Conclusion: In men with hypogonadism and cardiovascular disease (CVD) or increased risk of CVD, baseline and pre-COVID-19 on-treatment testosterone, dihydrotestosterone, and estradiol levels were similar in those who developed COVID-19 and those who did not. TRT did not affect the risk of COVID-19. COVID-19 attenuated the treatment response to TRT.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
