Baldev Singh, Nisha Kumari-Dewat, Adam Ryder, Vijay Klaire, Hannah Jennens, Kamran Ahmed, Mona Sidhu, Ananth Viswanath, Emma Parry
{"title":"Developing an electronic surprise question to predict end-of-life prognosis in a prospective cohort study of acute hospital admissions.","authors":"Baldev Singh, Nisha Kumari-Dewat, Adam Ryder, Vijay Klaire, Hannah Jennens, Kamran Ahmed, Mona Sidhu, Ananth Viswanath, Emma Parry","doi":"10.1016/j.clinme.2025.100292","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>Determining the accuracy of a method calculating the Gold Standards Framework Surprise Question (GSFSQ) equivalent end-of-life prognosis amongst hospital inpatients.</p><p><strong>Design: </strong>A prospective cohort study with regression calculated 1-year mortality probability. Probability cut points triaged unknown prognosis into the GSFSQ equivalent 'Yes' or 'No' survival categories (> or < 1-year respectively), with subsidiary classification of 'No'. Prediction was tested against prospective mortality.</p><p><strong>Setting: </strong>An acute NHS hospital.</p><p><strong>Participants: </strong>18,838 acute medical admissions.</p><p><strong>Interventions: </strong>Allocation of mortality probability by binary logistic regression model (X<sup>2</sup>=6,650.2, p<0.001, r<sup>2</sup> = 0.43) and stepwise algorithmic risk-stratification.</p><p><strong>Main outcome measure: </strong>Prospective mortality at 1-year.</p><p><strong>Results: </strong>End-of-life prognosis was unknown in 67.9%. The algorithm's prognosis allocation (100% vs baseline 32.1%) yielded cohorts of GSFSQ-Yes 15,264 (81%), GSFSQ-No Green 1,771 (9.4%) and GSFSQ-No Amber or Red 1,803 (9.6%). There were 5,043 (26.8%) deaths at 1-year. In Cox's survival, model allocated cohorts were discrete for mortality (GSFSQ-Yes 16.4% v GSFSQ-No 71.0% (p<0.001). For the GSFSQ-No classification, the mortality odds ratio was 12.4 (11.4-13.5) (p<0.001) vs GSFSQ-Yes (c-statistic 0.72 (0.70-0.73), p<0.001; accuracy, positive and negative predictive values 81.2%, 83.6%, 83.6%, respectively). Had the tool been utilised at the time of admission, the potential to reduce possibly avoidable subsequent hospital admissions, death-in-hospital and bed days was significant (p<0.001).</p><p><strong>Conclusion: </strong>This study is unique in methodology with prospectively evidenced outcomes. The model algorithm allocated GSFSQ equivalent EOL prognosis universally to a cohort of acutely admitted patients with statistical accuracy validated against prospective mortality outcomes.</p>","PeriodicalId":10492,"journal":{"name":"Clinical Medicine","volume":" ","pages":"100292"},"PeriodicalIF":3.9000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11907446/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinical Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1016/j.clinme.2025.100292","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/6 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: Determining the accuracy of a method calculating the Gold Standards Framework Surprise Question (GSFSQ) equivalent end-of-life prognosis amongst hospital inpatients.
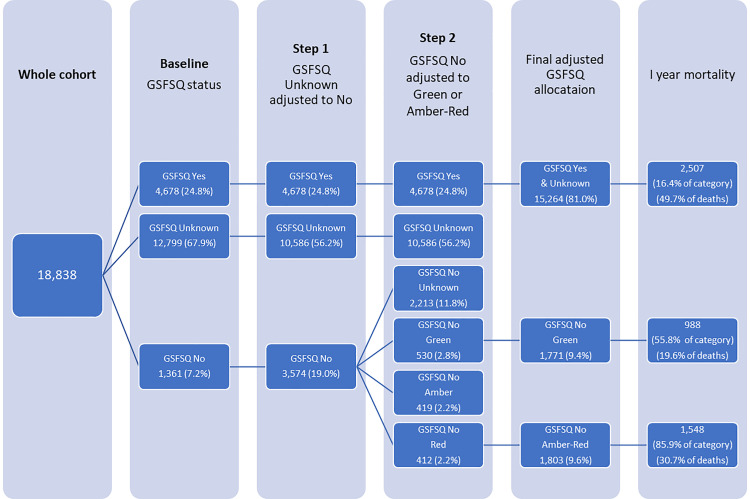
Design: A prospective cohort study with regression calculated 1-year mortality probability. Probability cut points triaged unknown prognosis into the GSFSQ equivalent 'Yes' or 'No' survival categories (> or < 1-year respectively), with subsidiary classification of 'No'. Prediction was tested against prospective mortality.
Setting: An acute NHS hospital.
Participants: 18,838 acute medical admissions.
Interventions: Allocation of mortality probability by binary logistic regression model (X2=6,650.2, p<0.001, r2 = 0.43) and stepwise algorithmic risk-stratification.
Main outcome measure: Prospective mortality at 1-year.
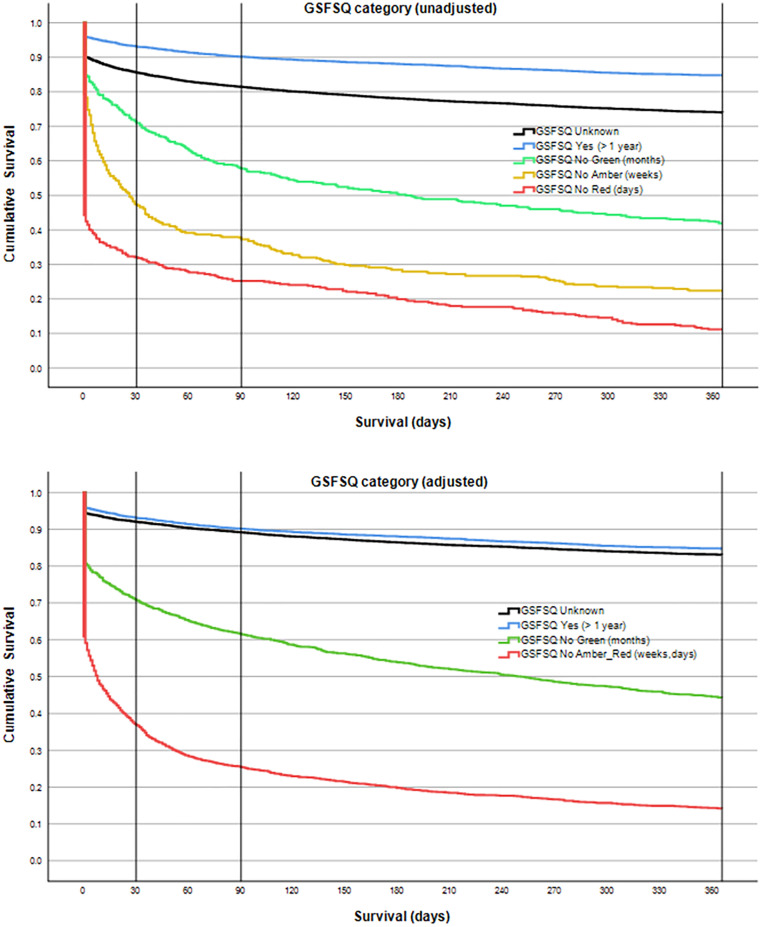
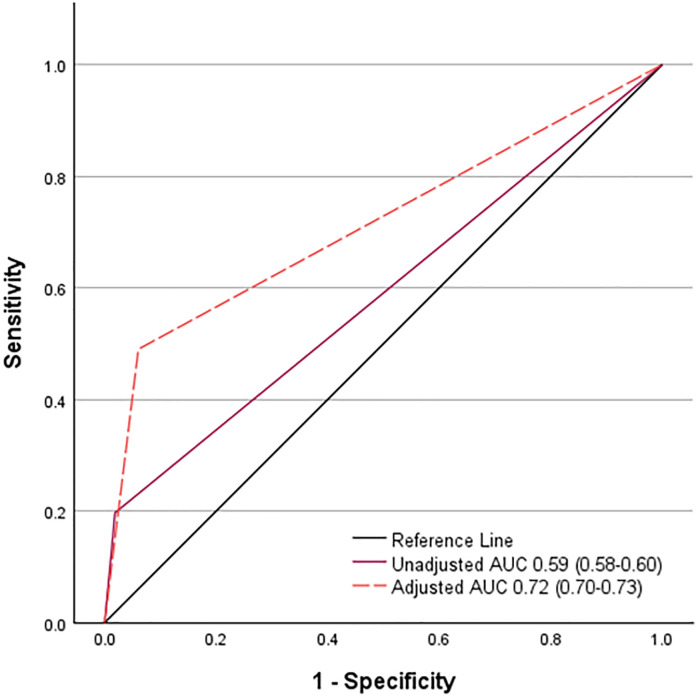
Results: End-of-life prognosis was unknown in 67.9%. The algorithm's prognosis allocation (100% vs baseline 32.1%) yielded cohorts of GSFSQ-Yes 15,264 (81%), GSFSQ-No Green 1,771 (9.4%) and GSFSQ-No Amber or Red 1,803 (9.6%). There were 5,043 (26.8%) deaths at 1-year. In Cox's survival, model allocated cohorts were discrete for mortality (GSFSQ-Yes 16.4% v GSFSQ-No 71.0% (p<0.001). For the GSFSQ-No classification, the mortality odds ratio was 12.4 (11.4-13.5) (p<0.001) vs GSFSQ-Yes (c-statistic 0.72 (0.70-0.73), p<0.001; accuracy, positive and negative predictive values 81.2%, 83.6%, 83.6%, respectively). Had the tool been utilised at the time of admission, the potential to reduce possibly avoidable subsequent hospital admissions, death-in-hospital and bed days was significant (p<0.001).
Conclusion: This study is unique in methodology with prospectively evidenced outcomes. The model algorithm allocated GSFSQ equivalent EOL prognosis universally to a cohort of acutely admitted patients with statistical accuracy validated against prospective mortality outcomes.
期刊介绍:
Clinical Medicine is aimed at practising physicians in the UK and overseas and has relevance to all those managing or working within the healthcare sector.
Available in print and online, the journal seeks to encourage high standards of medical care by promoting good clinical practice through original research, review and comment. The journal also includes a dedicated continuing medical education (CME) section in each issue. This presents the latest advances in a chosen specialty, with self-assessment questions at the end of each topic enabling CPD accreditation to be acquired.
ISSN: 1470-2118 E-ISSN: 1473-4893 Frequency: 6 issues per year



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
