Maria Carmen Viana, Alan E Kazdin, Meredith G Harris, Dan J Stein, Daniel V Vigo, Irving Hwang, Sophie M Manoukian, Nancy A Sampson, Jordi Alonso, Laura Helena Andrade, Guilherme Borges, Brendan Bunting, José Miguel Caldas-de-Almeida, Giovanni de Girolamo, Peter de Jonge, Oye Gureje, Josep Maria Haro, Elie G Karam, Viviane Kovess-Masfety, Jacek Moskalewicz, Fernando Navarro-Mateu, Daisuke Nishi, Marina Piazza, José Posada-Villa, Kate M Scott, Cristian Vladescu, Bogdan Wojtyniak, Zahari Zarkov, Ronald C Kessler, Timothy Kessler
{"title":"Barriers to 12-month treatment of common anxiety, mood, and substance use disorders in the World Mental Health (WMH) surveys.","authors":"Maria Carmen Viana, Alan E Kazdin, Meredith G Harris, Dan J Stein, Daniel V Vigo, Irving Hwang, Sophie M Manoukian, Nancy A Sampson, Jordi Alonso, Laura Helena Andrade, Guilherme Borges, Brendan Bunting, José Miguel Caldas-de-Almeida, Giovanni de Girolamo, Peter de Jonge, Oye Gureje, Josep Maria Haro, Elie G Karam, Viviane Kovess-Masfety, Jacek Moskalewicz, Fernando Navarro-Mateu, Daisuke Nishi, Marina Piazza, José Posada-Villa, Kate M Scott, Cristian Vladescu, Bogdan Wojtyniak, Zahari Zarkov, Ronald C Kessler, Timothy Kessler","doi":"10.1186/s13033-024-00658-2","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>High unmet need for treatment of mental disorders exists throughout the world. An understanding of barriers to treatment is needed to develop effective programs to address this problem.</p><p><strong>Methods: </strong>Data on barriers were obtained from face-to-face interviews in 22 community surveys across 19 countries (n = 102,812 respondents aged ≥ 18 years, 57.7% female, median age [interquartile range]: 43 [31-57] years; 68.5% weighted average response rate) in the World Mental Health (WMH) surveys. We focus on the n = 5,136 respondents with 12-month DSM-IV anxiety, mood, or substance use disorders with perceived need for treatment. The n = 2,444 such respondents who did not receive treatment were asked about barriers to receiving treatment, whereas the n = 926 respondents who received treatment with a delay were asked about barriers leading to delays. Consistent with previous research, we distinguished five broad classes of barriers: low perceived disorder severity, two types of barriers in the domain of predisposing factors (beliefs/attitudes about treatment ineffectiveness and stigma) and two types in the domain of enabling factors (financial and nonfinancial). Baseline predictors of receiving treatment found in a prior report (i.e., comparing the n = 2,692 respondents who received treatment with the n = 2,444 who did not) were examined as predictors of barriers, while barriers were examined as mediators of associations between these predictors and treatment.</p><p><strong>Results: </strong>Most respondents reported multiple barriers. Barriers among respondents who did not receive treatment included low perceived severity (52.9%), perceived treatment ineffectiveness (44.8%), nonfinancial (40.2%) and financial (32.9%) barriers in the domain of enabling factors, and stigma (20.6%). Barriers causing delays in treatment had a similar rank-order but were reported by higher proportions of respondents (X<sup>2</sup><sub>1</sub> = 3.8-199.8, p = 0.050- < 0.001). Barriers were predicted by low education, disorder type, age, employment status, and financial obstacles. Predictors varied as a function of barrier type.</p><p><strong>Conclusions: </strong>A wide range of barriers to treatment exist among people with mental disorders even after a need for treatment is acknowledged. Most such individuals have multiple barriers. These results have important implications for the design of programs to decrease unmet need for treatment of mental disorders.</p>","PeriodicalId":47752,"journal":{"name":"International Journal of Mental Health Systems","volume":"19 1","pages":"6"},"PeriodicalIF":3.8000,"publicationDate":"2025-02-09","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11807321/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International Journal of Mental Health Systems","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13033-024-00658-2","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"PSYCHIATRY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: High unmet need for treatment of mental disorders exists throughout the world. An understanding of barriers to treatment is needed to develop effective programs to address this problem.
Methods: Data on barriers were obtained from face-to-face interviews in 22 community surveys across 19 countries (n = 102,812 respondents aged ≥ 18 years, 57.7% female, median age [interquartile range]: 43 [31-57] years; 68.5% weighted average response rate) in the World Mental Health (WMH) surveys. We focus on the n = 5,136 respondents with 12-month DSM-IV anxiety, mood, or substance use disorders with perceived need for treatment. The n = 2,444 such respondents who did not receive treatment were asked about barriers to receiving treatment, whereas the n = 926 respondents who received treatment with a delay were asked about barriers leading to delays. Consistent with previous research, we distinguished five broad classes of barriers: low perceived disorder severity, two types of barriers in the domain of predisposing factors (beliefs/attitudes about treatment ineffectiveness and stigma) and two types in the domain of enabling factors (financial and nonfinancial). Baseline predictors of receiving treatment found in a prior report (i.e., comparing the n = 2,692 respondents who received treatment with the n = 2,444 who did not) were examined as predictors of barriers, while barriers were examined as mediators of associations between these predictors and treatment.
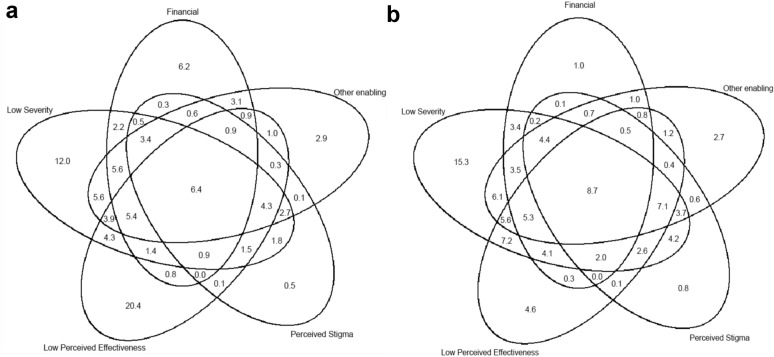
Results: Most respondents reported multiple barriers. Barriers among respondents who did not receive treatment included low perceived severity (52.9%), perceived treatment ineffectiveness (44.8%), nonfinancial (40.2%) and financial (32.9%) barriers in the domain of enabling factors, and stigma (20.6%). Barriers causing delays in treatment had a similar rank-order but were reported by higher proportions of respondents (X21 = 3.8-199.8, p = 0.050- < 0.001). Barriers were predicted by low education, disorder type, age, employment status, and financial obstacles. Predictors varied as a function of barrier type.
Conclusions: A wide range of barriers to treatment exist among people with mental disorders even after a need for treatment is acknowledged. Most such individuals have multiple barriers. These results have important implications for the design of programs to decrease unmet need for treatment of mental disorders.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
