Combined PD-1 and CTLA-4 Blockade Increases the Risks of Multiple Pituitary Hormone Deficiency and Isolated Adrenocorticotropic Deficiency: A Prospective Study.
{"title":"Combined PD-1 and CTLA-4 Blockade Increases the Risks of Multiple Pituitary Hormone Deficiency and Isolated Adrenocorticotropic Deficiency: A Prospective Study.","authors":"Shintaro Iwama, Tomoko Kobayashi, Tetsushi Izuchi, Koji Suzuki, Takanori Murase, Masahiko Ando, Tomoko Handa, Takeshi Onoue, Takashi Miyata, Mariko Sugiyama, Daisuke Hagiwara, Hidetaka Suga, Ryoichi Banno, Tetsunari Hase, Shoichiro Mori, Tomoyasu Sano, Shusuke Akamatsu, Masashi Akiyama, Makoto Ishii, Hiroshi Arima","doi":"10.3803/EnM.2024.2180","DOIUrl":null,"url":null,"abstract":"<p><strong>Backgruound: </strong>Anti-cytotoxic T-lymphocyte antigen-4 antibody (CTLA-4-Ab) monotherapy induces two types of pituitary immunerelated adverse events (irAEs): multiple pituitary hormone deficiency (Multi-D; impairment of ≥2 anterior pituitary hormones) and isolated adrenocorticotropic hormone (ACTH) deficiency (IAD). Combination therapy with CTLA-4-Ab and anti-programmed cell death-1 antibody (PD-1/CTLA-4-Abs), which is increasingly replacing CTLA-4-Ab monotherapy, frequently causes pituitary irAEs; however, whether it increases Multi-D/IAD incidence is unknown.</p><p><strong>Methods: </strong>In total, 74 and 748 patients with malignancies treated with PD-1/CTLA-4-Abs and PD-1-Ab, respectively, were prospectively evaluated for ACTH and cortisol levels at baseline and every 6 weeks after treatment initiation, and then observed until the last clinical visit. The characteristics of pituitary irAEs were evaluated by pituitary stimulation tests and compared with those induced by PD-1-Ab monotherapy.</p><p><strong>Results: </strong>PD-1/CTLA-4-Abs therapy showed higher incidence rates of pituitary irAEs (16/74 [21.6%] vs. 25/748 [3.3%], P<0.001), Multi-D (9/74 [12.2%] vs. 2/748 [0.3%], P<0.001), and IAD (7/74 [9.5%] vs. 23/748 [3.1%], P=0.014) than PD-1-Ab monotherapy. ACTH deficiency was observed in all cases, whereas the prevalence rates of luteinizing hormone deficiency (8/16 [50.0%] vs. 1/25 [4.0%]), follicle-stimulating hormone deficiency (6/16 [37.5%] vs. 1/25 [4.0%]), and thyrotropin deficiency (4/16 [25.0%] vs. 0/25 [0%]) were significantly higher after PD-1/CTLA-4-Abs than after PD-1-Ab treatment. Pituitary enlargement, which was observed only in the Multi-D cases, was significantly more frequent after PD-1/CTLA-4-Abs than after PD-1-Ab treatment (6/16 [37.5%] vs. 0/25 [0%], P=0.002).</p><p><strong>Conclusion: </strong>This prospective study revealed high risks of both Multi-D and IAD under PD-1/CTLA-4-Abs treatment, emphasizing the need for careful evaluation of pituitary function.</p>","PeriodicalId":11636,"journal":{"name":"Endocrinology and Metabolism","volume":" ","pages":"459-468"},"PeriodicalIF":4.2000,"publicationDate":"2025-06-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12230258/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrinology and Metabolism","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3803/EnM.2024.2180","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/11 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
Backgruound: Anti-cytotoxic T-lymphocyte antigen-4 antibody (CTLA-4-Ab) monotherapy induces two types of pituitary immunerelated adverse events (irAEs): multiple pituitary hormone deficiency (Multi-D; impairment of ≥2 anterior pituitary hormones) and isolated adrenocorticotropic hormone (ACTH) deficiency (IAD). Combination therapy with CTLA-4-Ab and anti-programmed cell death-1 antibody (PD-1/CTLA-4-Abs), which is increasingly replacing CTLA-4-Ab monotherapy, frequently causes pituitary irAEs; however, whether it increases Multi-D/IAD incidence is unknown.
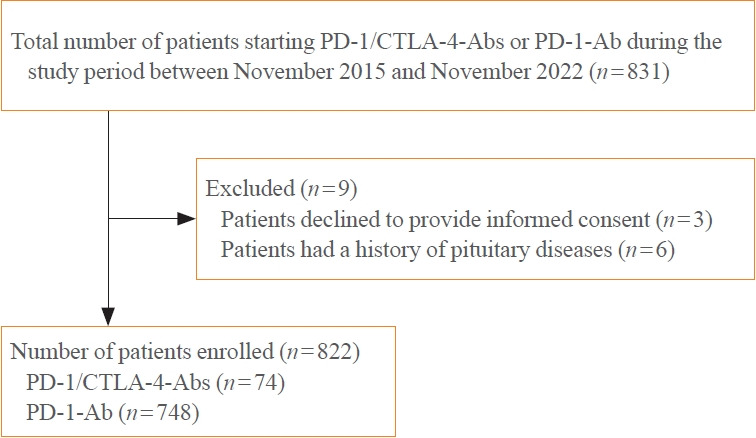
Methods: In total, 74 and 748 patients with malignancies treated with PD-1/CTLA-4-Abs and PD-1-Ab, respectively, were prospectively evaluated for ACTH and cortisol levels at baseline and every 6 weeks after treatment initiation, and then observed until the last clinical visit. The characteristics of pituitary irAEs were evaluated by pituitary stimulation tests and compared with those induced by PD-1-Ab monotherapy.
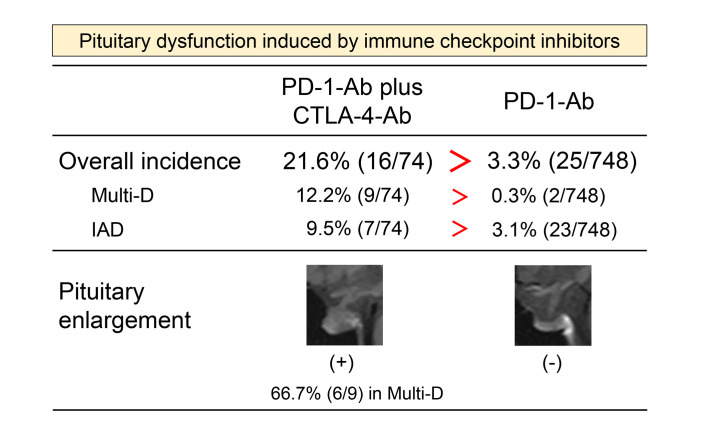
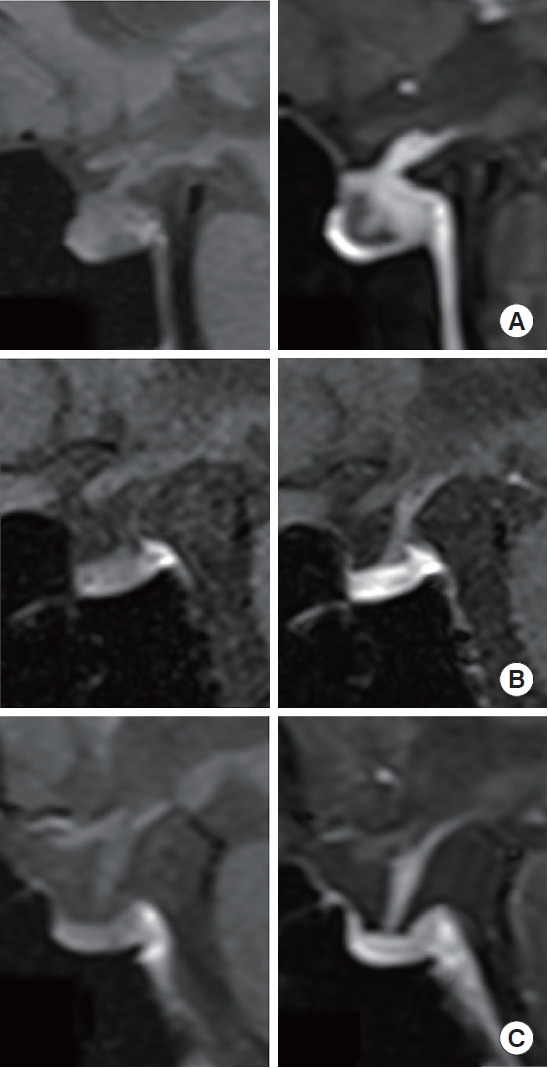
Results: PD-1/CTLA-4-Abs therapy showed higher incidence rates of pituitary irAEs (16/74 [21.6%] vs. 25/748 [3.3%], P<0.001), Multi-D (9/74 [12.2%] vs. 2/748 [0.3%], P<0.001), and IAD (7/74 [9.5%] vs. 23/748 [3.1%], P=0.014) than PD-1-Ab monotherapy. ACTH deficiency was observed in all cases, whereas the prevalence rates of luteinizing hormone deficiency (8/16 [50.0%] vs. 1/25 [4.0%]), follicle-stimulating hormone deficiency (6/16 [37.5%] vs. 1/25 [4.0%]), and thyrotropin deficiency (4/16 [25.0%] vs. 0/25 [0%]) were significantly higher after PD-1/CTLA-4-Abs than after PD-1-Ab treatment. Pituitary enlargement, which was observed only in the Multi-D cases, was significantly more frequent after PD-1/CTLA-4-Abs than after PD-1-Ab treatment (6/16 [37.5%] vs. 0/25 [0%], P=0.002).
Conclusion: This prospective study revealed high risks of both Multi-D and IAD under PD-1/CTLA-4-Abs treatment, emphasizing the need for careful evaluation of pituitary function.
期刊介绍:
The aim of this journal is to set high standards of medical care by providing a forum for discussion for basic, clinical, and translational researchers and clinicians on new findings in the fields of endocrinology and metabolism. Endocrinology and Metabolism reports new findings and developments in all aspects of endocrinology and metabolism. The topics covered by this journal include bone and mineral metabolism, cytokines, developmental endocrinology, diagnostic endocrinology, endocrine research, dyslipidemia, endocrine regulation, genetic endocrinology, growth factors, hormone receptors, hormone action and regulation, management of endocrine diseases, clinical trials, epidemiology, molecular endocrinology, neuroendocrinology, neuropeptides, neurotransmitters, obesity, pediatric endocrinology, reproductive endocrinology, signal transduction, the anatomy and physiology of endocrine organs (i.e., the pituitary, thyroid, parathyroid, and adrenal glands, and the gonads), and endocrine diseases (diabetes, nutrition, osteoporosis, etc.).



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
