{"title":"Patient-ventilator synchrony under non-invasive ventilation is improved by an automated real time waveform analysis algorithm: a bench study.","authors":"Yann Renaud, Jocelyne Auroi, Davy Cabrio, Ermes Lupieri, Jean-Daniel Chiche, Lise Piquilloud","doi":"10.1186/s40635-025-00726-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Because of inherent leaks, obtaining good patient-ventilator synchrony during non-invasive ventilation (NIV) is challenging. The IntelliSync + <sup>®</sup> software (Hamilton medical, Bonaduz, CH), that can be used together with the NIV mode, performs real-time automated analysis of airway pressure- and flow-time curves to detect the transition between inspiration and expiration. It then controls the ventilator inspiratory and expiratory valves to improve patient-ventilator synchrony. The main goal of this NIV bench study was to evaluate the impact of IntelliSync + <sup>®</sup> on synchrony in the presence of leaks of 9 and 20 L/min in the tested ventilator circuit (no face mask used), with normal, obstructive and restrictive respiratory mechanics and two levels of NIV pressure support (PS 8 and 14 cmH<sub>2</sub>O). For this, the time needed to trigger the ventilator (Td) and the difference between the end of the simulated breath and the termination of pressurization (Tiex) were measured. The number of classical asynchronies and the ventilator pressurization capacity were also assessed.</p><p><strong>Results: </strong>Compared to NIV delivered with the classical NIV mode (compensating leaks and limiting inspiratory time to 2 s), activating IntelliSync + <sup>®</sup> improved Tiex and, to a lesser extent, Td in clinically relevant setups. IntelliSync + <sup>®</sup> also showed a trend towards reducing classical asynchronies, particularly directly after leak flow increase. The impact of the system was most significant with high PS levels and pathological respiratory mechanics. Especially, in the obstructive model, in the presence of large leak (20 L/min) and PS 14 cmH<sub>2</sub>O, Tiex decreased from 0.61 [0.56-0.64] to 0.16 [0.07-0.18] s and Td from 0.07 [0.06-0.08] to 0.06 [0.06-0.08] s. In less challenging situations, IntelliSync + <sup>®</sup> was less beneficial. Overall, ventilator pressurization was improved when IntelliSync + <sup>®</sup> was activated.</p><p><strong>Conclusions: </strong>In this NIV bench model, IntelliSync + <sup>®</sup>, used in addition to NIV-PS, improved both expiratory and inspiratory synchrony. It was particularly efficient in the presence of obstructive and restrictive respiratory mechanics and high-pressure support levels. These pre-clinical results tend to support the ability of IntelliSync + <sup>®</sup> to improve patient-ventilator synchrony in the presence of leaks and provide pre-clinical data supporting a clinical evaluation of the automated algorithm during NIV.</p>","PeriodicalId":13750,"journal":{"name":"Intensive Care Medicine Experimental","volume":"13 1","pages":"16"},"PeriodicalIF":2.8000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11822138/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Intensive Care Medicine Experimental","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s40635-025-00726-y","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"CRITICAL CARE MEDICINE","Score":null,"Total":0}
引用次数: 0
Abstract
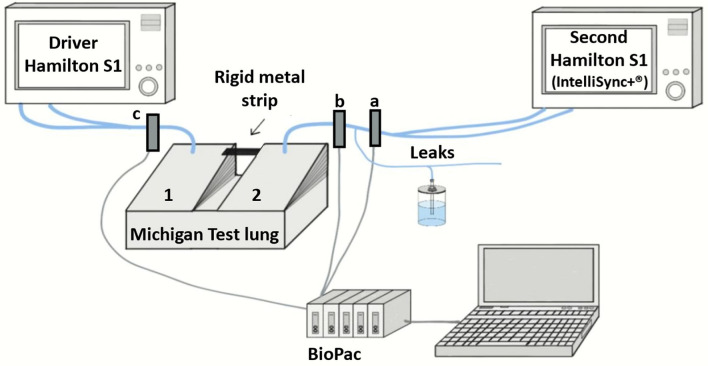
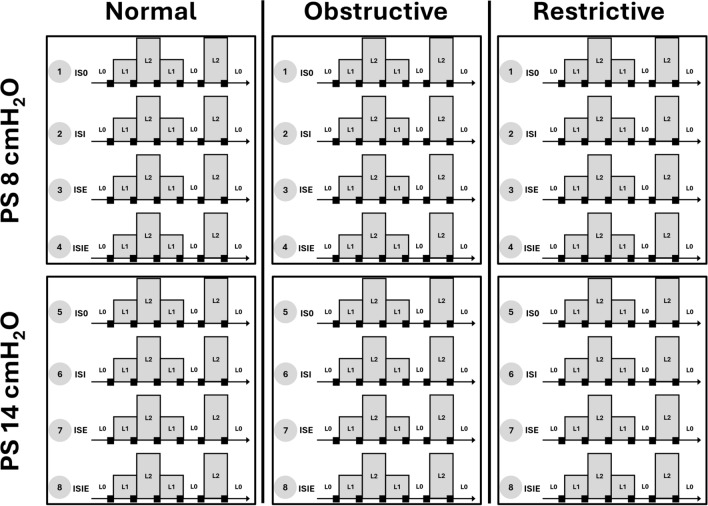
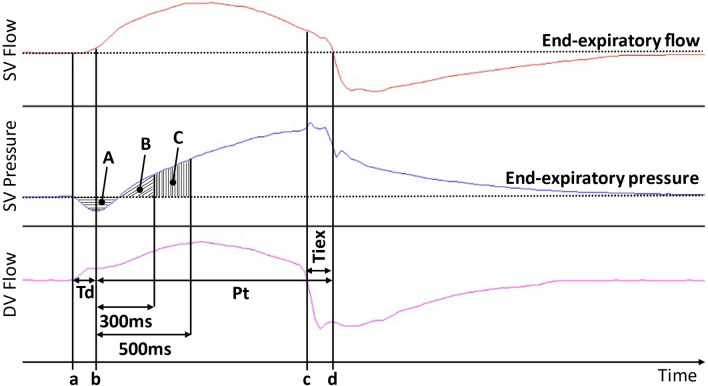
Background: Because of inherent leaks, obtaining good patient-ventilator synchrony during non-invasive ventilation (NIV) is challenging. The IntelliSync + ® software (Hamilton medical, Bonaduz, CH), that can be used together with the NIV mode, performs real-time automated analysis of airway pressure- and flow-time curves to detect the transition between inspiration and expiration. It then controls the ventilator inspiratory and expiratory valves to improve patient-ventilator synchrony. The main goal of this NIV bench study was to evaluate the impact of IntelliSync + ® on synchrony in the presence of leaks of 9 and 20 L/min in the tested ventilator circuit (no face mask used), with normal, obstructive and restrictive respiratory mechanics and two levels of NIV pressure support (PS 8 and 14 cmH2O). For this, the time needed to trigger the ventilator (Td) and the difference between the end of the simulated breath and the termination of pressurization (Tiex) were measured. The number of classical asynchronies and the ventilator pressurization capacity were also assessed.
Results: Compared to NIV delivered with the classical NIV mode (compensating leaks and limiting inspiratory time to 2 s), activating IntelliSync + ® improved Tiex and, to a lesser extent, Td in clinically relevant setups. IntelliSync + ® also showed a trend towards reducing classical asynchronies, particularly directly after leak flow increase. The impact of the system was most significant with high PS levels and pathological respiratory mechanics. Especially, in the obstructive model, in the presence of large leak (20 L/min) and PS 14 cmH2O, Tiex decreased from 0.61 [0.56-0.64] to 0.16 [0.07-0.18] s and Td from 0.07 [0.06-0.08] to 0.06 [0.06-0.08] s. In less challenging situations, IntelliSync + ® was less beneficial. Overall, ventilator pressurization was improved when IntelliSync + ® was activated.
Conclusions: In this NIV bench model, IntelliSync + ®, used in addition to NIV-PS, improved both expiratory and inspiratory synchrony. It was particularly efficient in the presence of obstructive and restrictive respiratory mechanics and high-pressure support levels. These pre-clinical results tend to support the ability of IntelliSync + ® to improve patient-ventilator synchrony in the presence of leaks and provide pre-clinical data supporting a clinical evaluation of the automated algorithm during NIV.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
