Kodavoor Shreesha Kumar, Raju Sumithra, S Tamilarasi, Dandapani Ramamurthy
{"title":"Star Can Vac Capsulorhexis in White Total Cataracts - A Retrospective Interventional Analysis.","authors":"Kodavoor Shreesha Kumar, Raju Sumithra, S Tamilarasi, Dandapani Ramamurthy","doi":"10.22336/rjo.2024.73","DOIUrl":null,"url":null,"abstract":"<p><strong>Aim: </strong>Completing circular uniform anterior capsulorhexis in intumescent white cataracts is challenging for all cataract surgeons. Numerous techniques have been described to get a circular capsulorhexis and prevent perpendicular linear tears in the anterior capsule.</p><p><strong>Methods: </strong>570 cases of white total cataracts were selected for this retrospective clinical study. In this technique of Star CanVac rhexis, the anterior lens capsule was nicked using a 26 G cystotome, and multiple centripetal tears were made in the center to create a small star-shaped opening. A vacuum was used to develop capsulorhexis, and a 25 G flat tip cannula attached to a 5 ml syringe half filled with balanced salt solution (BSS) was used to build capsulorhexis. The piston of the 5 ml syringe was withdrawn to create a vacuum to hold the free capsular flap. It was then directed circularly to get a round capsulorhexis. Oozing liquefied cortex was aspirated simultaneously with the same cannula.</p><p><strong>Results: </strong>This technique was successfully executed in 564 eyes. Six eyes had anterior capsular tears, 2 of which extended into the posterior capsule.</p><p><strong>Discussion: </strong>Intumescent cataracts often complicate the rhexis procedure due to increased lens volume and pressure. Over time, different methods have been refined to handle the pressure variation between the anterior chamber and the intralenticular area, such as mini-rhexis, double rhexis, sewing needle capsulotomy, and phaco capsulotomy. The primary goal of these procedures is to first reduce the elevated intralenticular pressure. Star CanVac capsulotomy facilitates equal pressure between the anterior chamber and the lenticular compartment, effectively reducing the risk of accidental capsular tears. Advantages of this approach include completing rhexis in one step, removing the liquefied cortex simultaneously, and relying on easily accessible instruments.</p><p><strong>Conclusion: </strong>Star CanVac capsulorhexis is an effective, safe, and alternative technique to conventional capsulorhexis in total white cataracts.</p>","PeriodicalId":94355,"journal":{"name":"Romanian journal of ophthalmology","volume":"68 4","pages":"404-408"},"PeriodicalIF":0.0000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11809841/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Romanian journal of ophthalmology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22336/rjo.2024.73","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Aim: Completing circular uniform anterior capsulorhexis in intumescent white cataracts is challenging for all cataract surgeons. Numerous techniques have been described to get a circular capsulorhexis and prevent perpendicular linear tears in the anterior capsule.
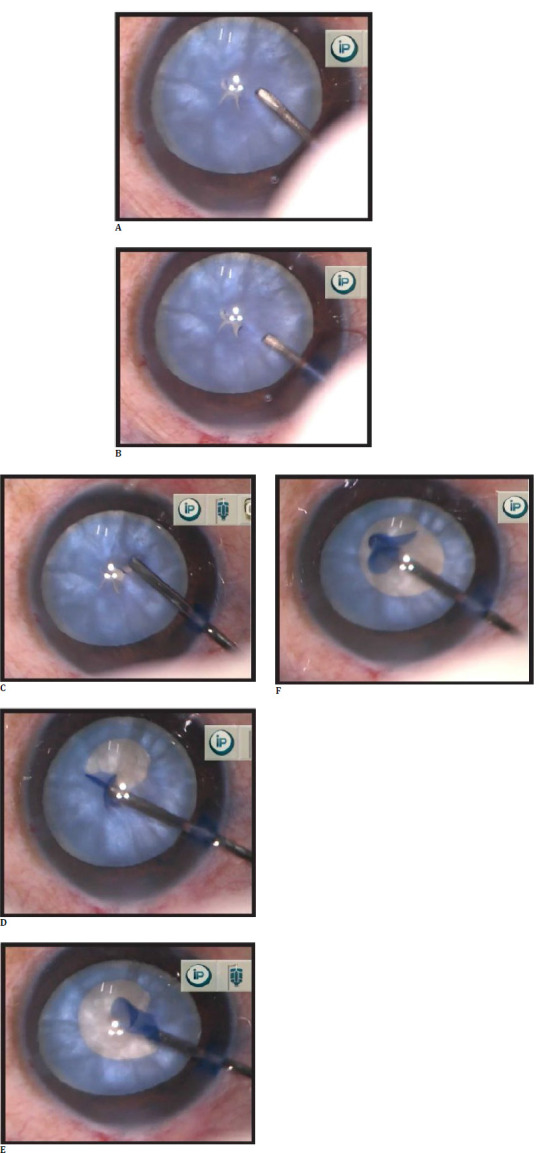
Methods: 570 cases of white total cataracts were selected for this retrospective clinical study. In this technique of Star CanVac rhexis, the anterior lens capsule was nicked using a 26 G cystotome, and multiple centripetal tears were made in the center to create a small star-shaped opening. A vacuum was used to develop capsulorhexis, and a 25 G flat tip cannula attached to a 5 ml syringe half filled with balanced salt solution (BSS) was used to build capsulorhexis. The piston of the 5 ml syringe was withdrawn to create a vacuum to hold the free capsular flap. It was then directed circularly to get a round capsulorhexis. Oozing liquefied cortex was aspirated simultaneously with the same cannula.
Results: This technique was successfully executed in 564 eyes. Six eyes had anterior capsular tears, 2 of which extended into the posterior capsule.
Discussion: Intumescent cataracts often complicate the rhexis procedure due to increased lens volume and pressure. Over time, different methods have been refined to handle the pressure variation between the anterior chamber and the intralenticular area, such as mini-rhexis, double rhexis, sewing needle capsulotomy, and phaco capsulotomy. The primary goal of these procedures is to first reduce the elevated intralenticular pressure. Star CanVac capsulotomy facilitates equal pressure between the anterior chamber and the lenticular compartment, effectively reducing the risk of accidental capsular tears. Advantages of this approach include completing rhexis in one step, removing the liquefied cortex simultaneously, and relying on easily accessible instruments.
Conclusion: Star CanVac capsulorhexis is an effective, safe, and alternative technique to conventional capsulorhexis in total white cataracts.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
