{"title":"Flecainide use in arrhythmic patients who have structural heart disease.","authors":"Naruepat Sangpornsuk, Voravut Rungpradubvong, Tachawut Tiensantisuk, Pattranee Leelapattana, Ronpichai Chokesuwattanakul, Somchai Prechawat","doi":"10.1177/20420986251316462","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Current guidelines recommend the use of only on a limited basis in patients with normal or minimal structural heart disease. The CAST study, the only randomized controlled trials, showed increased mortality from long-term flecainide use in post-myocardial infarction (MI) patients with reduced left ventricular ejection fraction (LVEF). However, many later studies have revealed its safety when used in other structural heart diseases.</p><p><strong>Objectives: </strong>This study investigates the incidence of ventricular tachycardia (VT) or ventricular fibrillation (VF) VT/VF in patients with structural heart disease compared to those with a normal heart when using flecainide.</p><p><strong>Methods: </strong>We retrospectively recruited patients who had received at least one dose of flecainide in the past 5 years. Baseline characteristics, indications for flecainide use, and echocardiography results were reviewed. After 1 year, we evaluated the incidence of ventricular arrhythmias and all-cause mortality.</p><p><strong>Results: </strong>After screening, 447 patients had received at least one dose of flecainide, and 336 patients were included in the study. Forty-seven patients (14%) had structural heart disease as defined by our protocols. Left ventricular hypertrophy (LVH) and impaired LVEF accounted for 28% and 25% of cases, respectively. There were five patients with coronary artery disease (CAD). After 1 year, ventricular arrhythmias occurred in two patients (4.7%) in the structural heart group; these patients had also experienced arrhythmias before receiving flecainide. In the non-structural heart group, ventricular arrhythmias were detected in three patients (1.1%). In multivariate analysis, structural heart disease was not associated with an increased incidence of ventricular arrhythmias (OR = 4.8 (0.6-38.44), <i>p</i> = 0.139).</p><p><strong>Conclusion: </strong>Our study showed that no patients died due to ventricular arrhythmia, and the incidence of VT/VF was not increased in patients with structural heart disease. A prospective study is needed to further evaluate the safety of flecainide in patients with structural heart disease other than ischemic heart disease.</p>","PeriodicalId":23012,"journal":{"name":"Therapeutic Advances in Drug Safety","volume":"16 ","pages":"20420986251316462"},"PeriodicalIF":3.4000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11815794/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Therapeutic Advances in Drug Safety","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/20420986251316462","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"PHARMACOLOGY & PHARMACY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Current guidelines recommend the use of only on a limited basis in patients with normal or minimal structural heart disease. The CAST study, the only randomized controlled trials, showed increased mortality from long-term flecainide use in post-myocardial infarction (MI) patients with reduced left ventricular ejection fraction (LVEF). However, many later studies have revealed its safety when used in other structural heart diseases.
Objectives: This study investigates the incidence of ventricular tachycardia (VT) or ventricular fibrillation (VF) VT/VF in patients with structural heart disease compared to those with a normal heart when using flecainide.
Methods: We retrospectively recruited patients who had received at least one dose of flecainide in the past 5 years. Baseline characteristics, indications for flecainide use, and echocardiography results were reviewed. After 1 year, we evaluated the incidence of ventricular arrhythmias and all-cause mortality.
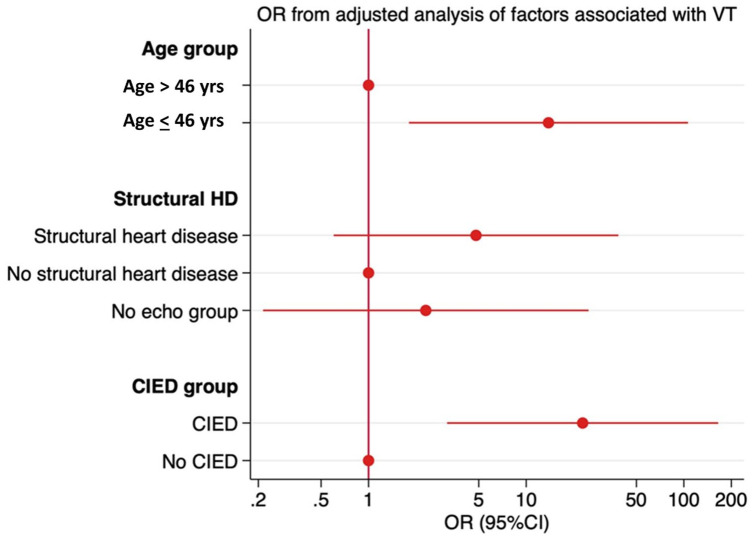
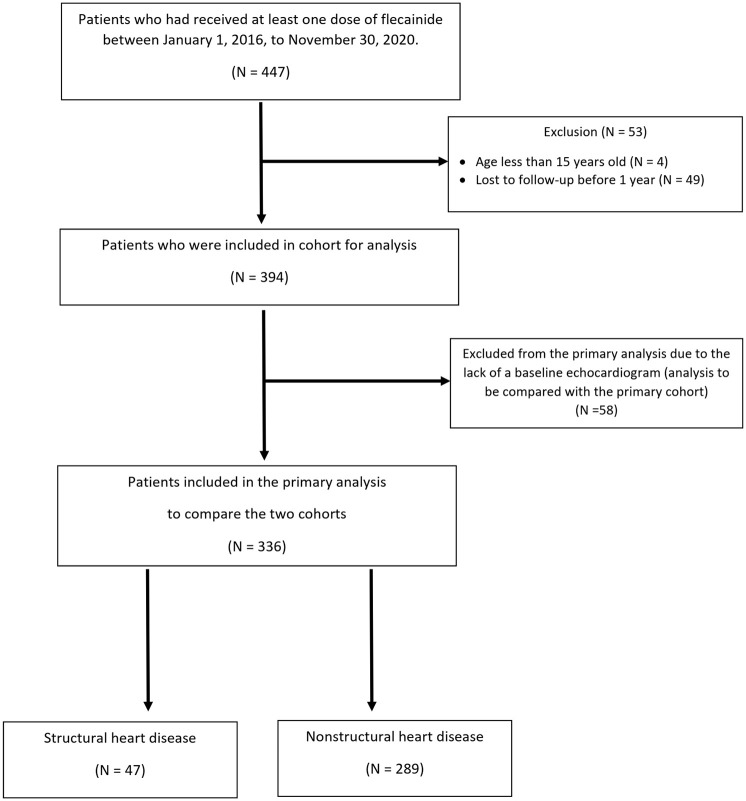
Results: After screening, 447 patients had received at least one dose of flecainide, and 336 patients were included in the study. Forty-seven patients (14%) had structural heart disease as defined by our protocols. Left ventricular hypertrophy (LVH) and impaired LVEF accounted for 28% and 25% of cases, respectively. There were five patients with coronary artery disease (CAD). After 1 year, ventricular arrhythmias occurred in two patients (4.7%) in the structural heart group; these patients had also experienced arrhythmias before receiving flecainide. In the non-structural heart group, ventricular arrhythmias were detected in three patients (1.1%). In multivariate analysis, structural heart disease was not associated with an increased incidence of ventricular arrhythmias (OR = 4.8 (0.6-38.44), p = 0.139).
Conclusion: Our study showed that no patients died due to ventricular arrhythmia, and the incidence of VT/VF was not increased in patients with structural heart disease. A prospective study is needed to further evaluate the safety of flecainide in patients with structural heart disease other than ischemic heart disease.
期刊介绍:
Therapeutic Advances in Drug Safety delivers the highest quality peer-reviewed articles, reviews, and scholarly comment on pioneering efforts and innovative studies pertaining to the safe use of drugs in patients.
The journal has a strong clinical and pharmacological focus and is aimed at clinicians and researchers in drug safety, providing a forum in print and online for publishing the highest quality articles in this area. The editors welcome articles of current interest on research across all areas of drug safety, including therapeutic drug monitoring, pharmacoepidemiology, adverse drug reactions, drug interactions, pharmacokinetics, pharmacovigilance, medication/prescribing errors, risk management, ethics and regulation.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
