Catherine G Derington, Ransmond O Berchie, Daniel O Scharfstein, Ryan M Andrews, Tom H Greene, Yizhe Xu, Jordan B King, Mark A Supiano, Joshua A Sonnen, Jeff Williamson, Nicholas M Pajewski, Jeremy J Pruzin, Jordana B Cohen, Adam P Bress
{"title":"Effect of Initiation and Continuous Adherence to ARBs Versus ACEIs on Risk of Adjudicated Mild Cognitive Impairment or Dementia.","authors":"Catherine G Derington, Ransmond O Berchie, Daniel O Scharfstein, Ryan M Andrews, Tom H Greene, Yizhe Xu, Jordan B King, Mark A Supiano, Joshua A Sonnen, Jeff Williamson, Nicholas M Pajewski, Jeremy J Pruzin, Jordana B Cohen, Adam P Bress","doi":"10.1093/gerona/glaf028","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Whether the differing mechanistic effects between angiotensin-2 receptor blockers (ARBs) and angiotensin-converting enzyme inhibitors (ACEIs) on the renin-angiotensin system translate to differential effects on clinical cognitive outcomes is unclear.</p><p><strong>Methods: </strong>We employed an active comparator, new-user cohort study to emulate a target trial evaluating the per-protocol effect of initiating and continuously adhering to an ARB versus ACEI on adjudicated amnestic mild cognitive impairment (MCI) and probable dementia (PD) in the Systolic Blood Pressure Intervention Trial (SPRINT). Inverse probability of treatment and censoring weighted cumulative incidence functions accounted for confounding, the competing risk of death, adherence, and loss to follow-up.</p><p><strong>Results: </strong>Of 9,361 SPRINT participants (mean age 67.1 ± 9.5 years, 36.7% female, 58.7% non-Hispanic White), 710 and 1,289 were new users of an ARB or ACEI. Overall, 291 (41.0%) ARB initiators and 854 (66.3%) ACEI initiators were nonadherent during follow-up. The IP-weighted 4-year probabilities of full adherence and being alive among ARB was 56.0% (95% CI: 52.2%-59.9%) and 30.5% (95% CI: 28.0%-33.1%) for ACEI. The 4-year weighted risk ratios (RR) for amnestic MCI/PD and for amnestic MCI/PD/death with initiation and full adherence to ARB versus ACEI were 0.94 (95% CI: 0.66-1.29) and 0.79 (95% CI: 0.58-1.06). The weighted 4-year weighted RR for all-cause death with ARB versus ACEI initiation and adherence was 0.36 (95% CI: 0.14-0.76).</p><p><strong>Conclusions: </strong>In this target trial emulation of older adults at high risk for cardiovascular disease, there was insufficient evidence to conclude a beneficial effect of initiating and continuously adhering to an ARB versus ACEI on adjudicated clinical cognitive outcomes.</p>","PeriodicalId":94243,"journal":{"name":"The journals of gerontology. Series A, Biological sciences and medical sciences","volume":" ","pages":""},"PeriodicalIF":0.0000,"publicationDate":"2025-06-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12287627/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"The journals of gerontology. Series A, Biological sciences and medical sciences","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1093/gerona/glaf028","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Whether the differing mechanistic effects between angiotensin-2 receptor blockers (ARBs) and angiotensin-converting enzyme inhibitors (ACEIs) on the renin-angiotensin system translate to differential effects on clinical cognitive outcomes is unclear.
Methods: We employed an active comparator, new-user cohort study to emulate a target trial evaluating the per-protocol effect of initiating and continuously adhering to an ARB versus ACEI on adjudicated amnestic mild cognitive impairment (MCI) and probable dementia (PD) in the Systolic Blood Pressure Intervention Trial (SPRINT). Inverse probability of treatment and censoring weighted cumulative incidence functions accounted for confounding, the competing risk of death, adherence, and loss to follow-up.
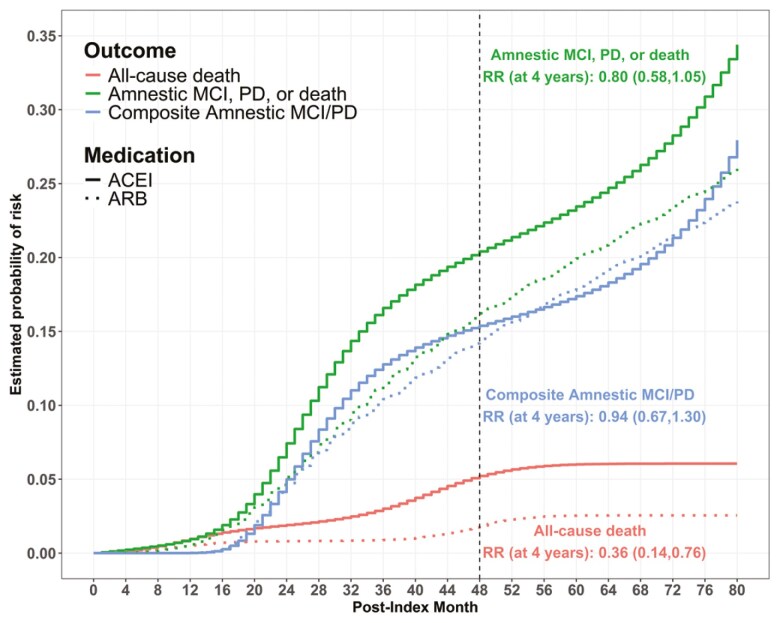
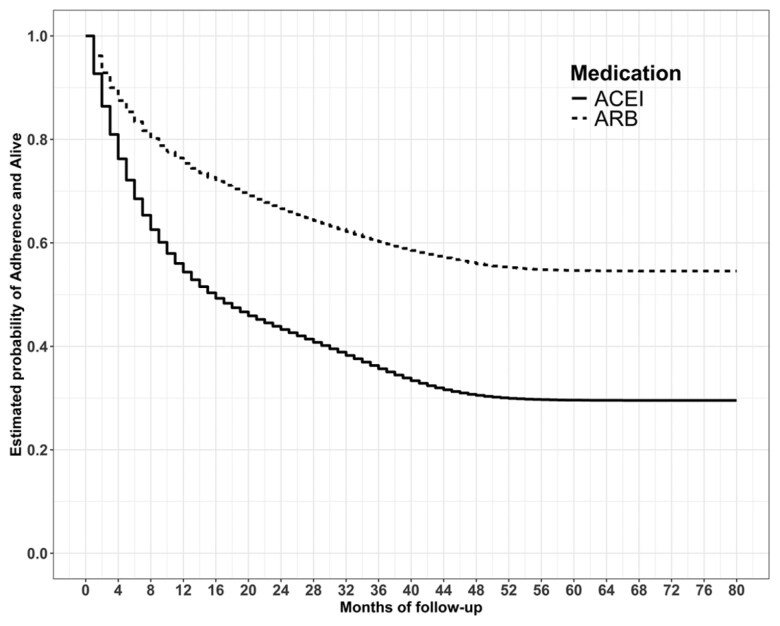
Results: Of 9,361 SPRINT participants (mean age 67.1 ± 9.5 years, 36.7% female, 58.7% non-Hispanic White), 710 and 1,289 were new users of an ARB or ACEI. Overall, 291 (41.0%) ARB initiators and 854 (66.3%) ACEI initiators were nonadherent during follow-up. The IP-weighted 4-year probabilities of full adherence and being alive among ARB was 56.0% (95% CI: 52.2%-59.9%) and 30.5% (95% CI: 28.0%-33.1%) for ACEI. The 4-year weighted risk ratios (RR) for amnestic MCI/PD and for amnestic MCI/PD/death with initiation and full adherence to ARB versus ACEI were 0.94 (95% CI: 0.66-1.29) and 0.79 (95% CI: 0.58-1.06). The weighted 4-year weighted RR for all-cause death with ARB versus ACEI initiation and adherence was 0.36 (95% CI: 0.14-0.76).
Conclusions: In this target trial emulation of older adults at high risk for cardiovascular disease, there was insufficient evidence to conclude a beneficial effect of initiating and continuously adhering to an ARB versus ACEI on adjudicated clinical cognitive outcomes.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
