Nisha Suda, Daisy Leon-Martinez, Patricia R Peter, Clare A Flannery, Roxanna A Irani
{"title":"Management of Severe Hypertriglyceridemia in Pregnancy With Niacin: Reevaluating Safety and Therapeutic Benefits.","authors":"Nisha Suda, Daisy Leon-Martinez, Patricia R Peter, Clare A Flannery, Roxanna A Irani","doi":"10.1155/crie/2644678","DOIUrl":null,"url":null,"abstract":"<p><p><b>Background:</b> Severe hypertriglyceridemia (triglycerides (TGs) >1000 mg/dL, >11.3 mmol/L) is a rare but potentially morbid condition in pregnancy. Physiological changes in pregnancy may unmask or exacerbate an underlying defect in TG metabolism. When conventional therapies are ineffective in controlling TG levels, a personalized management approach is needed. We present a case of severe hypertriglyceridemic pancreatitis successfully managed with niacin, a treatment that has seen limited use in pregnancy due to the paucity of available data. <b>Case Presentation:</b> A 29-year-old pregnant woman with a history of cholecystectomy and a prepregnancy BMI of 30.6 kg/m<sup>2</sup> presented at 12 weeks' gestation with acute pancreatitis and severe hypertriglyceridemia (6900 mg/dL, 77.9 mmol/L). After initial management with intravenous (IV) fluids, insulin infusion, and a low-fat diet, her TG levels improved. However, she was readmitted at 23 weeks' gestation with recurrent hypertriglyceridemia (2872 mg/dL, 32.4 mmol/L), requiring a more aggressive insulin regimen. Despite various interventions, including omega-3 fatty acids (O3FAs), fenofibrate, and central venous catheter insulin infusion, her TG levels remained elevated, necessitating early delivery at 34 weeks' gestation. Her postpartum recovery included continued TG management with fenofibrate and O3FAs. Four years later, during a second pregnancy, she presented with similar hypertriglyceridemia, managed with diet, metformin, fenofibrate, and insulin. Due to persistent hypertriglyceridemia (>3000 mg/dL, 33.9 mmol/L), niacin was added as an additional therapy and titrated to 2000 mg/day, which successfully sustained TG levels below 1000 mg/dL (11.3 mmol/L) through the remainder of her pregnancy. She delivered her second child via cesarean section at 35 weeks' gestation due to preeclampsia. Both children had developmental issues, with her first child diagnosed with attention-deficient hyperactivity disorder (ADHD) and her second child with autism spectrum disorder and motor delays. The patient was encouraged to remain on long-term management for her metabolic condition. <b>Conclusions:</b> Managing severe hypertriglyceridemia during pregnancy is challenging due to uncertainties about treatment efficacy and safety. Timely reduction of maternal TGs is essential to prevent complications and requires adjustments throughout pregnancy. This case demonstrates the effectiveness and safety of niacin, often underutilized due to perceived side effects, in managing severe hypertriglyceridemia in pregnancy when other treatments were inadequate.</p>","PeriodicalId":9621,"journal":{"name":"Case Reports in Endocrinology","volume":"2025 ","pages":"2644678"},"PeriodicalIF":0.9000,"publicationDate":"2025-01-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11824309/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Endocrinology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1155/crie/2644678","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ENDOCRINOLOGY & METABOLISM","Score":null,"Total":0}
引用次数: 0
Abstract
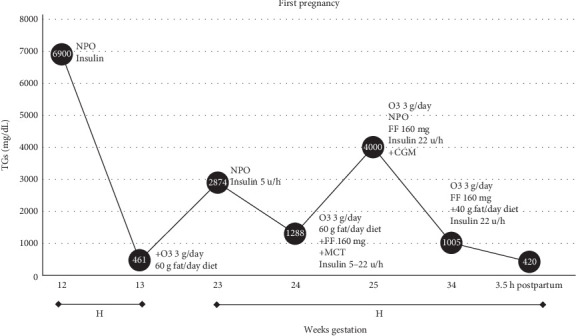
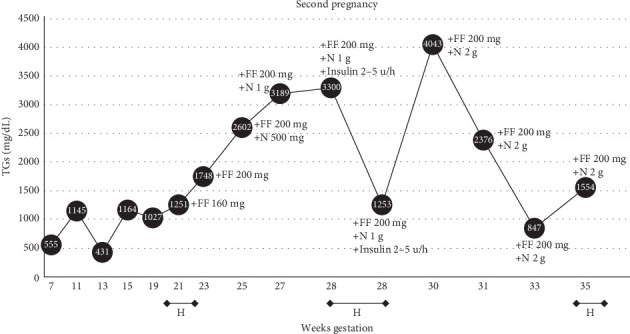
Background: Severe hypertriglyceridemia (triglycerides (TGs) >1000 mg/dL, >11.3 mmol/L) is a rare but potentially morbid condition in pregnancy. Physiological changes in pregnancy may unmask or exacerbate an underlying defect in TG metabolism. When conventional therapies are ineffective in controlling TG levels, a personalized management approach is needed. We present a case of severe hypertriglyceridemic pancreatitis successfully managed with niacin, a treatment that has seen limited use in pregnancy due to the paucity of available data. Case Presentation: A 29-year-old pregnant woman with a history of cholecystectomy and a prepregnancy BMI of 30.6 kg/m2 presented at 12 weeks' gestation with acute pancreatitis and severe hypertriglyceridemia (6900 mg/dL, 77.9 mmol/L). After initial management with intravenous (IV) fluids, insulin infusion, and a low-fat diet, her TG levels improved. However, she was readmitted at 23 weeks' gestation with recurrent hypertriglyceridemia (2872 mg/dL, 32.4 mmol/L), requiring a more aggressive insulin regimen. Despite various interventions, including omega-3 fatty acids (O3FAs), fenofibrate, and central venous catheter insulin infusion, her TG levels remained elevated, necessitating early delivery at 34 weeks' gestation. Her postpartum recovery included continued TG management with fenofibrate and O3FAs. Four years later, during a second pregnancy, she presented with similar hypertriglyceridemia, managed with diet, metformin, fenofibrate, and insulin. Due to persistent hypertriglyceridemia (>3000 mg/dL, 33.9 mmol/L), niacin was added as an additional therapy and titrated to 2000 mg/day, which successfully sustained TG levels below 1000 mg/dL (11.3 mmol/L) through the remainder of her pregnancy. She delivered her second child via cesarean section at 35 weeks' gestation due to preeclampsia. Both children had developmental issues, with her first child diagnosed with attention-deficient hyperactivity disorder (ADHD) and her second child with autism spectrum disorder and motor delays. The patient was encouraged to remain on long-term management for her metabolic condition. Conclusions: Managing severe hypertriglyceridemia during pregnancy is challenging due to uncertainties about treatment efficacy and safety. Timely reduction of maternal TGs is essential to prevent complications and requires adjustments throughout pregnancy. This case demonstrates the effectiveness and safety of niacin, often underutilized due to perceived side effects, in managing severe hypertriglyceridemia in pregnancy when other treatments were inadequate.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
