Thomas Roe, Alex Gordon, Nicholas Gourd, Charlotte Thomas, James Ward, Chinar Osman, Ahilanandan Dushianthan
{"title":"Immunoglobulin unresponsive Guillain-Barré syndrome: rinse or repeat? A systematic review.","authors":"Thomas Roe, Alex Gordon, Nicholas Gourd, Charlotte Thomas, James Ward, Chinar Osman, Ahilanandan Dushianthan","doi":"10.1136/bmjno-2024-000907","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Severe Guillain-Barré syndrome (GBS) patients may not show improvement after a single course of intravenous immunoglobulin (IVIg) therapy. Current treatment options include either a second course of IVIg or therapeutic plasma exchange (TPE). This systematic review aims to evaluate the current literature on the use of a second course of IVIg or TPE in patients who fail to show clinical improvement after the first IVIg course.</p><p><strong>Methods: </strong>We searched PubMed, Embase and Medline databases up until 26 October 2023. Studies that evaluated adult patients with confirmed GBS who have failed one full course of IVIg and subsequently received either repeat IVIg or TPE were included. Risk of bias was performed using study-specific checklists. A narrative synthesis of results is presented.</p><p><strong>Results: </strong>A total of 37 articles were identified (1 randomised controlled trial (RCT), 3 observational and 33 case reports/series), consisting of 422 patients in total. 12 studies evaluated repeat IVIg and 24 studies evaluated TPE after IVIg. There was no superiority of a repeat course of IVIg or TPE in all clinical outcome measures.</p><p><strong>Conclusions: </strong>The evidence suggests with a low degree of certainty that there is no beneficial effect of further IVIg in unresponsive GBS. The quality of evidence regarding TPE after IVIg is insufficient to suggest any efficacy due to a lack of RCTs. We recommend standardised case reporting with consideration for a multinational case registry and RCTs to determine the efficacy of TPE after initial IVIg unresponsiveness.</p>","PeriodicalId":52754,"journal":{"name":"BMJ Neurology Open","volume":"7 1","pages":"e000907"},"PeriodicalIF":2.4000,"publicationDate":"2025-02-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11822392/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Neurology Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjno-2024-000907","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Severe Guillain-Barré syndrome (GBS) patients may not show improvement after a single course of intravenous immunoglobulin (IVIg) therapy. Current treatment options include either a second course of IVIg or therapeutic plasma exchange (TPE). This systematic review aims to evaluate the current literature on the use of a second course of IVIg or TPE in patients who fail to show clinical improvement after the first IVIg course.
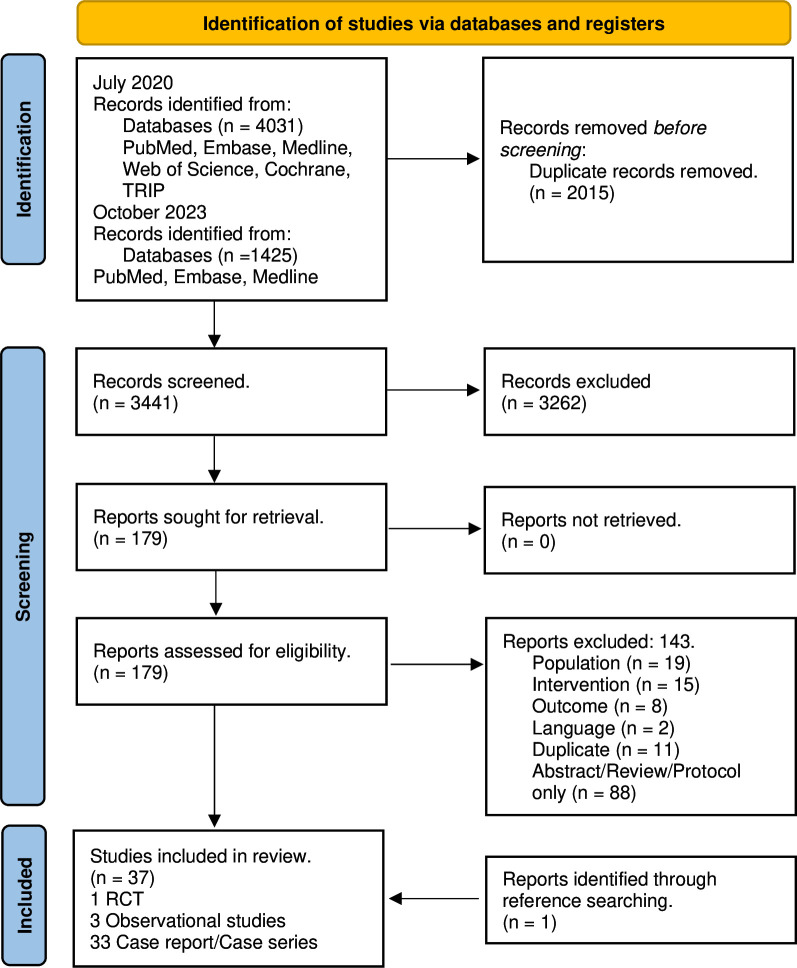
Methods: We searched PubMed, Embase and Medline databases up until 26 October 2023. Studies that evaluated adult patients with confirmed GBS who have failed one full course of IVIg and subsequently received either repeat IVIg or TPE were included. Risk of bias was performed using study-specific checklists. A narrative synthesis of results is presented.
Results: A total of 37 articles were identified (1 randomised controlled trial (RCT), 3 observational and 33 case reports/series), consisting of 422 patients in total. 12 studies evaluated repeat IVIg and 24 studies evaluated TPE after IVIg. There was no superiority of a repeat course of IVIg or TPE in all clinical outcome measures.
Conclusions: The evidence suggests with a low degree of certainty that there is no beneficial effect of further IVIg in unresponsive GBS. The quality of evidence regarding TPE after IVIg is insufficient to suggest any efficacy due to a lack of RCTs. We recommend standardised case reporting with consideration for a multinational case registry and RCTs to determine the efficacy of TPE after initial IVIg unresponsiveness.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
