William J Garvis, Blake A Johnson, Katherine E Kluesner, Stephanie M Garvis
{"title":"Characteristics of the Facial Canal-Lateral Canal Dehiscence: The Under-recognized Third Window.","authors":"William J Garvis, Blake A Johnson, Katherine E Kluesner, Stephanie M Garvis","doi":"10.1002/oto2.70085","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>We aimed to establish normative data on the bony partition between the facial canal (FC) and the lateral semicircular canal (LSCC) and present our initial series of cases in which an FC-LSCC dehiscence was identified based on these anatomic criteria, with or without other third window pathologies.</p><p><strong>Study design: </strong>Normative data: Analysis of archival otopathological human temporal bone specimens and computed tomography (CT) scans. Clinical data: Case studies.</p><p><strong>Setting: </strong>An otopathology laboratory and a specialized otolaryngology, head and neck surgery outpatient clinic.</p><p><strong>Methods: </strong>We measured the bony partition thickness between the FC-LSCC in human temporal bone otopathological specimens and CT scans. The clinical study involved a series of reviews of patients with FC-LSCC, presenting clinical data and CT images.</p><p><strong>Results: </strong>The average thickness of the bony partition measured via CT was 0.6 mm ± 0.2 mm, whereas in otopathological specimens it was 0.56 mm ± 0.17 mm. We identified 34 patients with FC-LSCC dehiscence. The most frequently reported symptoms were hearing loss (44%), dizziness/vertigo (44%), and tinnitus (41%). Of the patients, 15 (44%) had more than 1 site of bone dehiscence and 21 (62%) had bilateral FC-LSCC dehiscence. We then identified 36 patients in whom only FC-LSCC dehiscences were found and provided characteristics for this population.</p><p><strong>Conclusion: </strong>Our study provides normative characteristics on the bony partition between the FC-LSCC and the signs and symptoms of this third window abnormality. FC-LSCC should be included in differential diagnoses of patients presenting with third window syndrome symptoms.</p>","PeriodicalId":19697,"journal":{"name":"OTO Open","volume":"9 1","pages":"e70085"},"PeriodicalIF":1.8000,"publicationDate":"2025-02-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11831756/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"OTO Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1002/oto2.70085","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"OTORHINOLARYNGOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: We aimed to establish normative data on the bony partition between the facial canal (FC) and the lateral semicircular canal (LSCC) and present our initial series of cases in which an FC-LSCC dehiscence was identified based on these anatomic criteria, with or without other third window pathologies.
Study design: Normative data: Analysis of archival otopathological human temporal bone specimens and computed tomography (CT) scans. Clinical data: Case studies.
Setting: An otopathology laboratory and a specialized otolaryngology, head and neck surgery outpatient clinic.
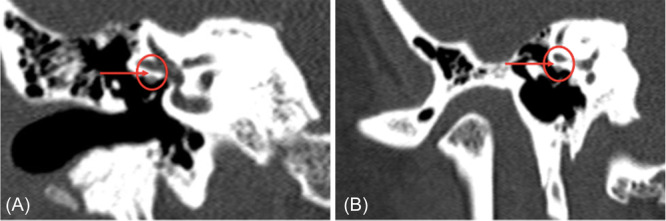
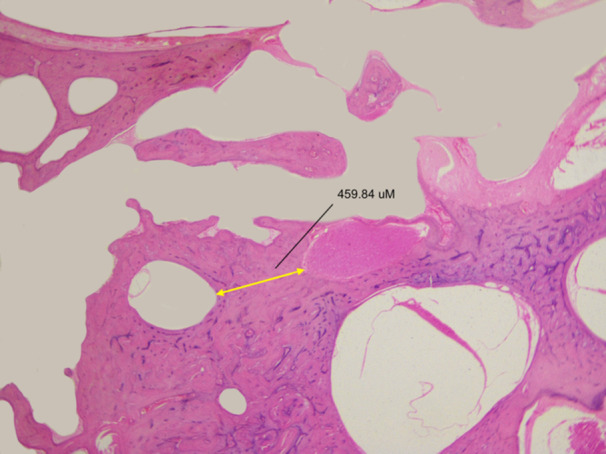
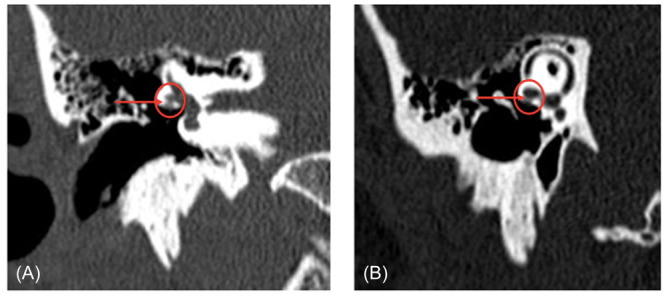
Methods: We measured the bony partition thickness between the FC-LSCC in human temporal bone otopathological specimens and CT scans. The clinical study involved a series of reviews of patients with FC-LSCC, presenting clinical data and CT images.
Results: The average thickness of the bony partition measured via CT was 0.6 mm ± 0.2 mm, whereas in otopathological specimens it was 0.56 mm ± 0.17 mm. We identified 34 patients with FC-LSCC dehiscence. The most frequently reported symptoms were hearing loss (44%), dizziness/vertigo (44%), and tinnitus (41%). Of the patients, 15 (44%) had more than 1 site of bone dehiscence and 21 (62%) had bilateral FC-LSCC dehiscence. We then identified 36 patients in whom only FC-LSCC dehiscences were found and provided characteristics for this population.
Conclusion: Our study provides normative characteristics on the bony partition between the FC-LSCC and the signs and symptoms of this third window abnormality. FC-LSCC should be included in differential diagnoses of patients presenting with third window syndrome symptoms.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
