Nita S. Kulkarni MD, Matthew P. Landler MD, Elaine R. Cohen MEd, Diane B. Wayne MD, Eytan Szmuilowicz MD
{"title":"Performance of electronic medical record tool in predicting 6-month mortality in hospitalized patients with cancer","authors":"Nita S. Kulkarni MD, Matthew P. Landler MD, Elaine R. Cohen MEd, Diane B. Wayne MD, Eytan Szmuilowicz MD","doi":"10.1002/jhm.70012","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>A systematic tool to identify hospitalized patients with high mortality risk may be beneficial for targeting palliative care to those in greatest need.</p>\n </section>\n \n <section>\n \n <h3> Objective</h3>\n \n <p>Evaluate the performance of the End-of-life Index (EOLI; Epic Systems Corporation) in identifying patients at the highest 6-month mortality risk among hospitalized patients with cancer.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We conducted a retrospective study of adults with cancer admitted to oncology services in a 959-bed hospital between July 1 and December 31, 2023. We evaluated EOLI score performance in determining mortality risk using the area under the receiver operating characteristic curve (AUC). The primary outcome was 6-month mortality for patients with an EOLI score above and below the optimal threshold value. Secondary outcomes included in-hospital mortality, 30-day mortality, length of stay, intensive care unit (ICU) utilization, palliative care consultation, do-not-resuscitate status on discharge, and discharge disposition.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The EOLI score had moderate accuracy in identifying patients at higher risk of 6-month mortality (AUC: 0.71) with an optimal threshold value of 40. For patients with EOLI > 40 and < 40, the 6-month mortality was 45.9% and 16.3%, respectively (<i>p</i> < .001). Patients with EOLI > 40 had higher ICU utilization (12.4% vs. 6.5%, <i>p</i> = .002) and were more likely to be discharged to a location other than home (13.5% vs. 5.3%; <i>p</i> < .001).</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>For hospitalized patients with cancer, the EOLI shows moderate accuracy in identifying patients with a high risk of 6-month mortality. As a screening tool, the EOLI can be used to identify patients who may benefit from timely palliative care.</p>\n </section>\n </div>","PeriodicalId":15883,"journal":{"name":"Journal of hospital medicine","volume":"20 8","pages":"829-836"},"PeriodicalIF":2.3000,"publicationDate":"2025-02-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jhm.70012","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of hospital medicine","FirstCategoryId":"3","ListUrlMain":"https://shmpublications.onlinelibrary.wiley.com/doi/10.1002/jhm.70012","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background
A systematic tool to identify hospitalized patients with high mortality risk may be beneficial for targeting palliative care to those in greatest need.
Objective
Evaluate the performance of the End-of-life Index (EOLI; Epic Systems Corporation) in identifying patients at the highest 6-month mortality risk among hospitalized patients with cancer.
Methods
We conducted a retrospective study of adults with cancer admitted to oncology services in a 959-bed hospital between July 1 and December 31, 2023. We evaluated EOLI score performance in determining mortality risk using the area under the receiver operating characteristic curve (AUC). The primary outcome was 6-month mortality for patients with an EOLI score above and below the optimal threshold value. Secondary outcomes included in-hospital mortality, 30-day mortality, length of stay, intensive care unit (ICU) utilization, palliative care consultation, do-not-resuscitate status on discharge, and discharge disposition.
Results
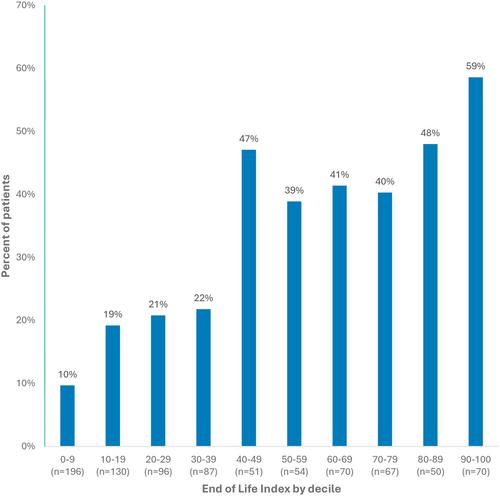
The EOLI score had moderate accuracy in identifying patients at higher risk of 6-month mortality (AUC: 0.71) with an optimal threshold value of 40. For patients with EOLI > 40 and < 40, the 6-month mortality was 45.9% and 16.3%, respectively (p < .001). Patients with EOLI > 40 had higher ICU utilization (12.4% vs. 6.5%, p = .002) and were more likely to be discharged to a location other than home (13.5% vs. 5.3%; p < .001).
Conclusions
For hospitalized patients with cancer, the EOLI shows moderate accuracy in identifying patients with a high risk of 6-month mortality. As a screening tool, the EOLI can be used to identify patients who may benefit from timely palliative care.
期刊介绍:
JHM is a peer-reviewed publication of the Society of Hospital Medicine and is published 12 times per year. JHM publishes manuscripts that address the care of hospitalized adults or children.
Broad areas of interest include (1) Treatments for common inpatient conditions; (2) Approaches to improving perioperative care; (3) Improving care for hospitalized patients with geriatric or pediatric vulnerabilities (such as mobility problems, or those with complex longitudinal care); (4) Evaluation of innovative healthcare delivery or educational models; (5) Approaches to improving the quality, safety, and value of healthcare across the acute- and postacute-continuum of care; and (6) Evaluation of policy and payment changes that affect hospital and postacute care.






 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
