Restriction of Posterior Tibial Translation During the Posterior Drawer Test in Internal or External Rotation Is Dependent on Peripheral Stabilizers of the Knee: A Biomechanical Robotic Investigation.
Adrian Deichsel, Christian Peez, Wenke Liu, Michael J Raschke, Alina Albert, Thorben Briese, Elmar Herbst, Christoph Kittl
{"title":"Restriction of Posterior Tibial Translation During the Posterior Drawer Test in Internal or External Rotation Is Dependent on Peripheral Stabilizers of the Knee: A Biomechanical Robotic Investigation.","authors":"Adrian Deichsel, Christian Peez, Wenke Liu, Michael J Raschke, Alina Albert, Thorben Briese, Elmar Herbst, Christoph Kittl","doi":"10.1177/03635465251317209","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The posteromedial and posterolateral structures of the knee have previously been shown to be secondary restraints to posterior tibial translation (PTT). The effect of these structures may increase when performing the posterior drawer test in internal or external rotation.</p><p><strong>Purpose/hypothesis: </strong>The purpose was to investigate the influence of the posteromedial and posterolateral structures on restricting PTT in neutral, external, and internal rotation. It was hypothesized that the posteromedial structures restrict PTT in internal rotation, while the posterolateral structures restrict PTT in external rotation.</p><p><strong>Study design: </strong>Controlled laboratory study.</p><p><strong>Methods: </strong>A sequential cutting study was performed on 24 fresh-frozen human knee specimens utilizing a 6 degrees of freedom robotic test setup. After determining the native knee kinematics from 0° to 90° of knee flexion, an 89-N posterior drawer test in neutral, internal, and external rotation was performed at 0°, 30°, 60°, and 90° of knee flexion. In 8 knees, a motion-controlled protocol was applied, replicating the native motion while the force was measured. The reduction of the restraining force represented the percentage contribution of each cut. In 16 knees, a force-controlled protocol was applied, determining the increase in PTT after each cut. After calculating the native knee kinematics, the posterior cruciate ligament (PCL) was cut, followed by randomized sectioning of the posteromedial (medial collateral ligament, posterior oblique ligament) and posterolateral (lateral collateral ligament, popliteus complex) structures. Mixed linear models with the post hoc Dunn test were used for statistical analysis.</p><p><strong>Results: </strong>During motion-controlled testing, performing the posterior drawer test in internal or external rotation significantly decreased the contribution of the PCL in restraining PTT. The PCL was the primary restraint to PTT during the posterior drawer test in neutral rotation at all flexion angles (24.4%-61.2% contribution). The primary restraint to PTT during the posterior drawer test in internal rotation was the posterior oblique ligament at 0° (24.2% ± 14.1%), the medial collateral ligament at 30° (33.6% ± 11.4%), and the PCL at 60° and 90° (46.2%-57.8%). In external rotation, the primary restraint was the lateral collateral ligament at 0° (24.7% ± 10.5%) and the popliteus complex at 30° to 90° (56.4%-65.2%). During force-controlled testing, PTT in the PCL-deficient knee was significantly decreased when performing the posterior drawer test in internal or external rotation. Insufficiency of the posterolateral or posteromedial structures, in addition to insufficiency of the PCL, during the posterior drawer test in neutral rotation led to an additional significant increase in PTT of up to 7.6 mm (95% confidence interval [CI], 3.6-11.7). Insufficiency of the posterolateral structures led to a significant further increase in PTT during the posterior drawer test in external rotation of up to 12.6 mm (95% CI, 3.5-21.8). Insufficiency of the posteromedial structures led to a significant additional increase in PTT during the posterior drawer test in internal rotation of up to 14.9 mm (95% CI, 8.2-21.6).</p><p><strong>Conclusion: </strong>The peripheral ligamentous structures of the knee acted as secondary restraints to PTT in neutral rotation and became primary stabilizers in internal or external rotation, depending on the flexion angle.</p><p><strong>Clinical relevance: </strong>This study may guide the clinician in diagnosing deficiencies of the posteromedial or posterolateral structures of the knee. In cases of isolated PCL deficiencies, PTT is reduced when the posterior drawer test is performed in internal or external rotation. However, an additional deficiency of the posteromedial or posterolateral structures further increases PTT.</p>","PeriodicalId":55528,"journal":{"name":"American Journal of Sports Medicine","volume":" ","pages":"1077-1084"},"PeriodicalIF":4.5000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11951389/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Sports Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1177/03635465251317209","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/19 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The posteromedial and posterolateral structures of the knee have previously been shown to be secondary restraints to posterior tibial translation (PTT). The effect of these structures may increase when performing the posterior drawer test in internal or external rotation.
Purpose/hypothesis: The purpose was to investigate the influence of the posteromedial and posterolateral structures on restricting PTT in neutral, external, and internal rotation. It was hypothesized that the posteromedial structures restrict PTT in internal rotation, while the posterolateral structures restrict PTT in external rotation.
Study design: Controlled laboratory study.
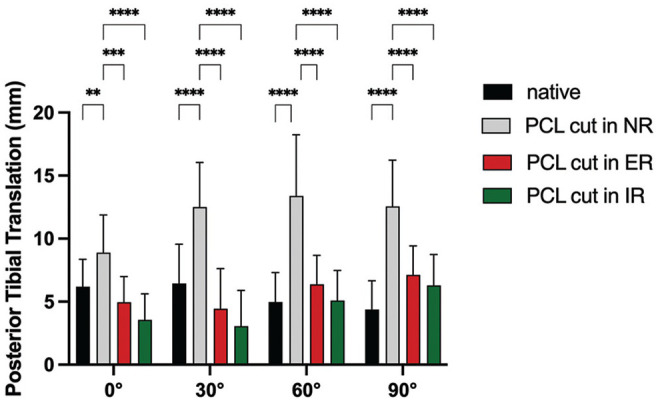
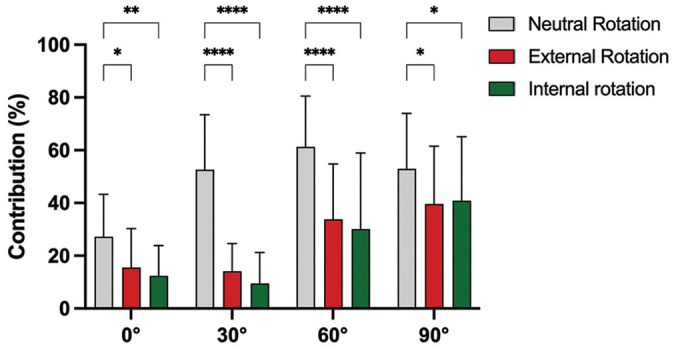
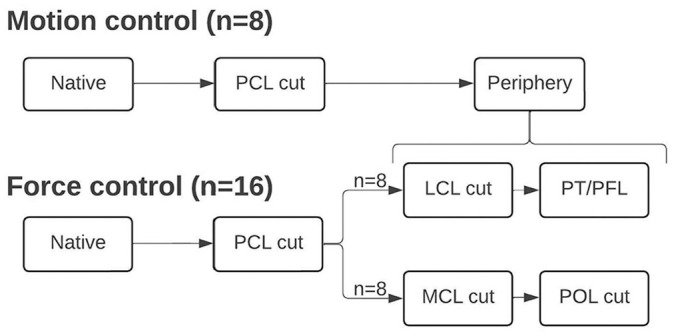
Methods: A sequential cutting study was performed on 24 fresh-frozen human knee specimens utilizing a 6 degrees of freedom robotic test setup. After determining the native knee kinematics from 0° to 90° of knee flexion, an 89-N posterior drawer test in neutral, internal, and external rotation was performed at 0°, 30°, 60°, and 90° of knee flexion. In 8 knees, a motion-controlled protocol was applied, replicating the native motion while the force was measured. The reduction of the restraining force represented the percentage contribution of each cut. In 16 knees, a force-controlled protocol was applied, determining the increase in PTT after each cut. After calculating the native knee kinematics, the posterior cruciate ligament (PCL) was cut, followed by randomized sectioning of the posteromedial (medial collateral ligament, posterior oblique ligament) and posterolateral (lateral collateral ligament, popliteus complex) structures. Mixed linear models with the post hoc Dunn test were used for statistical analysis.
Results: During motion-controlled testing, performing the posterior drawer test in internal or external rotation significantly decreased the contribution of the PCL in restraining PTT. The PCL was the primary restraint to PTT during the posterior drawer test in neutral rotation at all flexion angles (24.4%-61.2% contribution). The primary restraint to PTT during the posterior drawer test in internal rotation was the posterior oblique ligament at 0° (24.2% ± 14.1%), the medial collateral ligament at 30° (33.6% ± 11.4%), and the PCL at 60° and 90° (46.2%-57.8%). In external rotation, the primary restraint was the lateral collateral ligament at 0° (24.7% ± 10.5%) and the popliteus complex at 30° to 90° (56.4%-65.2%). During force-controlled testing, PTT in the PCL-deficient knee was significantly decreased when performing the posterior drawer test in internal or external rotation. Insufficiency of the posterolateral or posteromedial structures, in addition to insufficiency of the PCL, during the posterior drawer test in neutral rotation led to an additional significant increase in PTT of up to 7.6 mm (95% confidence interval [CI], 3.6-11.7). Insufficiency of the posterolateral structures led to a significant further increase in PTT during the posterior drawer test in external rotation of up to 12.6 mm (95% CI, 3.5-21.8). Insufficiency of the posteromedial structures led to a significant additional increase in PTT during the posterior drawer test in internal rotation of up to 14.9 mm (95% CI, 8.2-21.6).
Conclusion: The peripheral ligamentous structures of the knee acted as secondary restraints to PTT in neutral rotation and became primary stabilizers in internal or external rotation, depending on the flexion angle.
Clinical relevance: This study may guide the clinician in diagnosing deficiencies of the posteromedial or posterolateral structures of the knee. In cases of isolated PCL deficiencies, PTT is reduced when the posterior drawer test is performed in internal or external rotation. However, an additional deficiency of the posteromedial or posterolateral structures further increases PTT.
期刊介绍:
An invaluable resource for the orthopaedic sports medicine community, _The American Journal of Sports Medicine_ is a peer-reviewed scientific journal, first published in 1972. It is the official publication of the [American Orthopaedic Society for Sports Medicine (AOSSM)](http://www.sportsmed.org/)! The journal acts as an important forum for independent orthopaedic sports medicine research and education, allowing clinical practitioners the ability to make decisions based on sound scientific information.
This journal is a must-read for:
* Orthopaedic Surgeons and Specialists
* Sports Medicine Physicians
* Physiatrists
* Athletic Trainers
* Team Physicians
* And Physical Therapists


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
