Innovative Payment Models for Sickle-Cell Disease Gene Therapies in Medicaid: Leveraging Real-World Data and Insights from CMMI's Gene Therapy Access Model.
Antal Zemplenyi, Jim Leonard, Garth C Wright, Michael J DiStefano, Kavita Nair, Kelly E Anderson, R Brett McQueen
{"title":"Innovative Payment Models for Sickle-Cell Disease Gene Therapies in Medicaid: Leveraging Real-World Data and Insights from CMMI's Gene Therapy Access Model.","authors":"Antal Zemplenyi, Jim Leonard, Garth C Wright, Michael J DiStefano, Kavita Nair, Kelly E Anderson, R Brett McQueen","doi":"10.1007/s40273-025-01474-3","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>This study aims to evaluate the financial implications of implementing various payment models, including outcome-based agreements (OBAs), volume-based rebates, and guaranteed rebates, for the newly approved gene therapies, exagamglogene autotemcel (exa-cel) and lovotibeglogene autotemcel (lovo-cel), in the treatment of sickle-cell disease (SCD) from the perspective of Colorado Medicaid. The analysis specifically examines the cost of standard of care (SoC) for severe SCD, the impact of different eligibility criteria based on vaso-occlusive events (VOEs), and the potential financial impacts associated with rebate structures.</p><p><strong>Methods: </strong>Data from the Colorado Department of Health Care Policy & Financing (HCPF) database was used to estimate the annual costs for Medicaid-enrolled patients with severe SCD from 2018 to 2023. Patients were selected based on various eligibility criteria, including the number of VOEs, acute chest syndrome events, and stroke diagnoses. Three-state Markov models (SCD, stable, and dead) were constructed to compare the costs of SoC and gene therapies. The durability of gene therapy effectiveness and the financial impact of OBAs, volume-based rebates, and guaranteed rebates were evaluated over a 6-year contract period, with scenarios reflecting different VOE criteria and treatment durability.</p><p><strong>Results: </strong>The average annual SoC cost for severe SCD patients (N = 138) was US$45,941 (SD US$59,653), with higher costs associated with more frequent VOEs. Gene therapies exa-cel and lovo-cel, with one-off list prices of US$2.2 million and US$3.1 million, respectively, exhibited high upfront costs, resulting in a negative cumulative balance averaging - US$2.11 million for exa-cel and - US$3.00 million for lovo-cel per patient over 6 years compared with SoC. Outcome-based rebates could potentially save Medicaid approximately US$260K (uncertainty interval 88K-772K) per patient on average for exa-cel and US$367K (uncertainty interval 122K-1111K) for lovo-cel after they pay the full up-front cost. Volume-based and guaranteed rebates also offered potential savings but varied in impact based on contract duration and effectiveness of gene therapy.</p><p><strong>Conclusions: </strong>The study highlights critical considerations for Medicaid in negotiating OBAs for SCD gene therapies. Achieving budget neutrality over 6 years is unlikely due to low SoC costs. However, payment models can enhance value-based spending by linking high therapy costs and potential rebates to the health gains these treatments may offer. OBAs offer offsets contingent on therapy effectiveness durability and contract terms (such as length and price), while varying eligibility criteria impact budgets and outcomes. Medicaid real-world data is crucial for navigating complexities in defining eligible populations and structuring OBAs.</p>","PeriodicalId":19807,"journal":{"name":"PharmacoEconomics","volume":" ","pages":"583-594"},"PeriodicalIF":4.6000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12011968/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"PharmacoEconomics","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s40273-025-01474-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/21 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ECONOMICS","Score":null,"Total":0}
引用次数: 0
Abstract
Objective: This study aims to evaluate the financial implications of implementing various payment models, including outcome-based agreements (OBAs), volume-based rebates, and guaranteed rebates, for the newly approved gene therapies, exagamglogene autotemcel (exa-cel) and lovotibeglogene autotemcel (lovo-cel), in the treatment of sickle-cell disease (SCD) from the perspective of Colorado Medicaid. The analysis specifically examines the cost of standard of care (SoC) for severe SCD, the impact of different eligibility criteria based on vaso-occlusive events (VOEs), and the potential financial impacts associated with rebate structures.
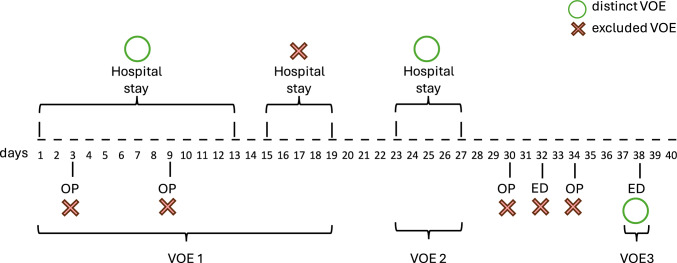
Methods: Data from the Colorado Department of Health Care Policy & Financing (HCPF) database was used to estimate the annual costs for Medicaid-enrolled patients with severe SCD from 2018 to 2023. Patients were selected based on various eligibility criteria, including the number of VOEs, acute chest syndrome events, and stroke diagnoses. Three-state Markov models (SCD, stable, and dead) were constructed to compare the costs of SoC and gene therapies. The durability of gene therapy effectiveness and the financial impact of OBAs, volume-based rebates, and guaranteed rebates were evaluated over a 6-year contract period, with scenarios reflecting different VOE criteria and treatment durability.
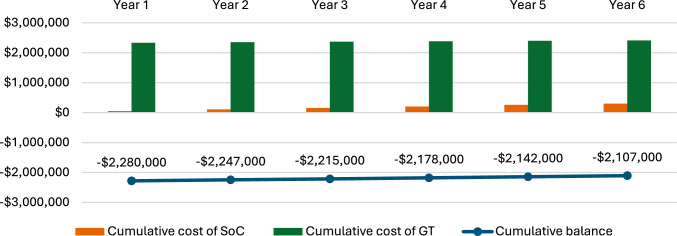
Results: The average annual SoC cost for severe SCD patients (N = 138) was US$45,941 (SD US$59,653), with higher costs associated with more frequent VOEs. Gene therapies exa-cel and lovo-cel, with one-off list prices of US$2.2 million and US$3.1 million, respectively, exhibited high upfront costs, resulting in a negative cumulative balance averaging - US$2.11 million for exa-cel and - US$3.00 million for lovo-cel per patient over 6 years compared with SoC. Outcome-based rebates could potentially save Medicaid approximately US$260K (uncertainty interval 88K-772K) per patient on average for exa-cel and US$367K (uncertainty interval 122K-1111K) for lovo-cel after they pay the full up-front cost. Volume-based and guaranteed rebates also offered potential savings but varied in impact based on contract duration and effectiveness of gene therapy.
Conclusions: The study highlights critical considerations for Medicaid in negotiating OBAs for SCD gene therapies. Achieving budget neutrality over 6 years is unlikely due to low SoC costs. However, payment models can enhance value-based spending by linking high therapy costs and potential rebates to the health gains these treatments may offer. OBAs offer offsets contingent on therapy effectiveness durability and contract terms (such as length and price), while varying eligibility criteria impact budgets and outcomes. Medicaid real-world data is crucial for navigating complexities in defining eligible populations and structuring OBAs.
期刊介绍:
PharmacoEconomics is the benchmark journal for peer-reviewed, authoritative and practical articles on the application of pharmacoeconomics and quality-of-life assessment to optimum drug therapy and health outcomes. An invaluable source of applied pharmacoeconomic original research and educational material for the healthcare decision maker.
PharmacoEconomics is dedicated to the clear communication of complex pharmacoeconomic issues related to patient care and drug utilization.
PharmacoEconomics offers a range of additional features designed to increase the visibility, readership and educational value of the journal’s content. Each article is accompanied by a Key Points summary, giving a time-efficient overview of the content to a wide readership. Articles may be accompanied by plain language summaries to assist readers who have some knowledge of, but not in-depth expertise in, the area to understand the scientific content and overall implications of the article.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
