{"title":"Budget Impact and Cost-Benefit Analyses of Sodium-Glucose Cotransporter-2 Inhibitors for Patients With Heart Failure in Thailand.","authors":"Poukwan Arunmanakul, Tuangrat Phodha, Sakkarin Pinta-Ay, Mantiwee Nimworapan, Arintaya Phrommintikul, Noppakun Thammatacharee, Piyameth Dilokthornsakul","doi":"10.2147/CEOR.S504819","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>To assess the budget impact and cost-benefit of incorporating sodium-glucose cotransporter-2 inhibitors (SGLT-2i) into the benefit package for patients with heart failure (HF) under the universal health coverage (UHC) in Thailand.</p><p><strong>Patients and methods: </strong>A budget impact analysis and cost-benefit model were developed using a five-year time horizon from the payer perspective. Dapagliflozin 10 mg daily or Empagliflozin 10 mg daily was considered as an additional treatment to standard of care (SoC) for patients with HF, under the UHC. Two analytical frameworks were applied: (1) only medicine cost and (2) medicine cost and cost of hospitalization for HF (HHF) and urinary tract infection (UTI) admission as the adverse event of SGLT-2i. The net budget impacts (NBI) were calculated along with the HHF cost reduction and benefit-cost ratio.</p><p><strong>Results: </strong>The NBI in the first year in only medicine cost for dapagliflozin was 12,535 million Thai baht (THB) and that for empagliflozin was 13,265 million THB. The NBIs, when considering HHF and UTI admission costs, were 7661 and 7407 million THB in the first year. The prices of dapagliflozin and empagliflozin should be reduced by 57.13% and 52.07% to reach a budget impact of 500 million THB. The benefit-cost ratio was 0.396 for dapagliflozin and 0.456 for empagliflozin.</p><p><strong>Conclusion: </strong>Incorporating SGLT-2i into the UHC would significantly impact the healthcare budget. Policymakers should consider this valuable evidence.</p>","PeriodicalId":47313,"journal":{"name":"ClinicoEconomics and Outcomes Research","volume":"17 ","pages":"95-105"},"PeriodicalIF":2.2000,"publicationDate":"2025-02-17","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11844265/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"ClinicoEconomics and Outcomes Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/CEOR.S504819","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"HEALTH CARE SCIENCES & SERVICES","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: To assess the budget impact and cost-benefit of incorporating sodium-glucose cotransporter-2 inhibitors (SGLT-2i) into the benefit package for patients with heart failure (HF) under the universal health coverage (UHC) in Thailand.
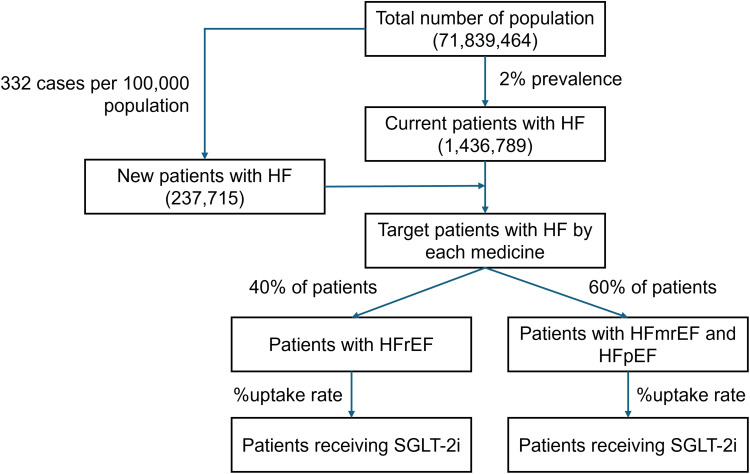
Patients and methods: A budget impact analysis and cost-benefit model were developed using a five-year time horizon from the payer perspective. Dapagliflozin 10 mg daily or Empagliflozin 10 mg daily was considered as an additional treatment to standard of care (SoC) for patients with HF, under the UHC. Two analytical frameworks were applied: (1) only medicine cost and (2) medicine cost and cost of hospitalization for HF (HHF) and urinary tract infection (UTI) admission as the adverse event of SGLT-2i. The net budget impacts (NBI) were calculated along with the HHF cost reduction and benefit-cost ratio.
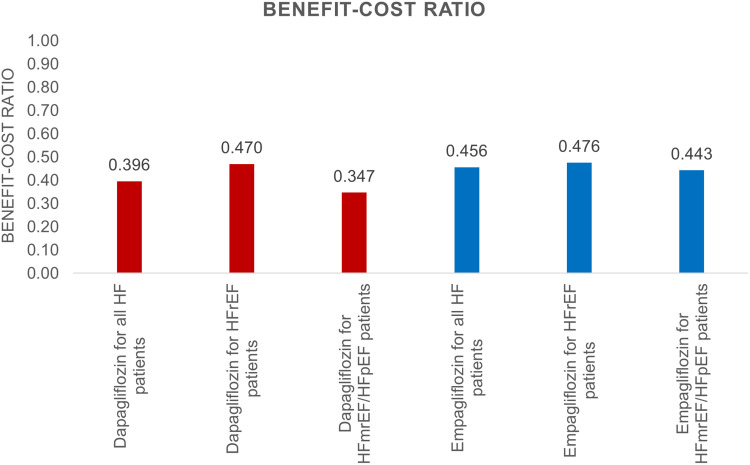
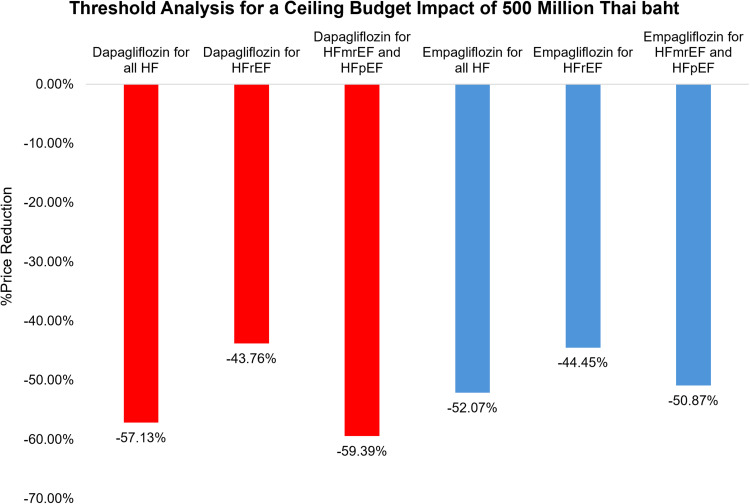
Results: The NBI in the first year in only medicine cost for dapagliflozin was 12,535 million Thai baht (THB) and that for empagliflozin was 13,265 million THB. The NBIs, when considering HHF and UTI admission costs, were 7661 and 7407 million THB in the first year. The prices of dapagliflozin and empagliflozin should be reduced by 57.13% and 52.07% to reach a budget impact of 500 million THB. The benefit-cost ratio was 0.396 for dapagliflozin and 0.456 for empagliflozin.
Conclusion: Incorporating SGLT-2i into the UHC would significantly impact the healthcare budget. Policymakers should consider this valuable evidence.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
