The role of co-infections and hormonal contraceptives in cervical intraepithelial neoplasia prevalence among women referred to a tertiary hospital in Western Kenya.
Calleb George Onyango, Lilian Ogonda, Bernard Guyah
{"title":"The role of co-infections and hormonal contraceptives in cervical intraepithelial neoplasia prevalence among women referred to a tertiary hospital in Western Kenya.","authors":"Calleb George Onyango, Lilian Ogonda, Bernard Guyah","doi":"10.1186/s13027-024-00620-4","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Screening for co-infections with HIV, HSV-2 and Chlamydia trachomatis (CT) among high-risk human papilloma virus (hr-HPV) positive women, coupled with enhanced counseling on contraceptives use remains essential in alleviating high morbidity of cervical cancer (CC). The aim of this study was to determine the prevalence of cervical intraepithelial neoplasia (CIN) among women referred for CC screening at a referral hospital in Kisumu County, Kenya; and to establish the role of co-infection and hormonal contraceptives on CIN.</p><p><strong>Method: </strong>In a cross-sectional study, we collected HPV, HIV, HSV-2 and CT data, cervical cytology results, and demographic information from 517 referrals. Blood samples were obtained for HIV and HSV-2 tests; urine for CT test, cervical swabs for hr-HPV test and colposcopic biopsy for histology confirmation after visual inspection with acetic acid (VIA).</p><p><strong>Results: </strong>The overall prevalence of CIN was 18.4% (95/517) with CIN1 observed in 56(29.6%), CIN2 in 27(`14.3%), CIN3 and above (CIN3+) in 12(6.3%) and normal biopsy in 94(49.7%) of the patients out of which high grade CIN2 and above (CIN2+) was 7.54% (39/517) equivalent to 32.5 per 100,000 women per year. In a univariate analysis; HPV/HIV co-infection (infected vs. uninfected: OR 2.79; 95% CI 1.56-5.10, p < 0.001); HPV/HSV-2 co-infection (infected vs. uninfected: OR 2.41; 95% CI: 1.12-5.46, p < 0.024); HPV/CT co-infection (infected vs. uninfected: OR 3.83; 95% CI 1.84-8.51, p < 0.001) were found to be significantly associated with CIN. Additionally, hormone-containing intra uterine device (HIUD) contraceptives (users vs. none users: OR 1.43; 95% CI 0.28-10.9, p < 0.017) were also associated with CIN.</p><p><strong>Conclusion: </strong>Co-infections with HIV, HSV-2 or Chlamydia trachomatis and use of HIUD were associated with increased risk of testing positive for CIN in HPV positive women. Although the overall prevalence of CIN was high, high-grade CIN2 + was comparable to the rates reported earlier. Therefore, population screening for co-infections alongside hr-HPV is desirable and is likely to reduce the burden of CIN in the region. Besides, women positive for hr-HPV and opting for contraceptives ought to be counseled about the possible positive and negative side-effects of different contraception options.</p>","PeriodicalId":13568,"journal":{"name":"Infectious Agents and Cancer","volume":"20 1","pages":"11"},"PeriodicalIF":2.8000,"publicationDate":"2025-02-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11853817/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Infectious Agents and Cancer","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13027-024-00620-4","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"IMMUNOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Screening for co-infections with HIV, HSV-2 and Chlamydia trachomatis (CT) among high-risk human papilloma virus (hr-HPV) positive women, coupled with enhanced counseling on contraceptives use remains essential in alleviating high morbidity of cervical cancer (CC). The aim of this study was to determine the prevalence of cervical intraepithelial neoplasia (CIN) among women referred for CC screening at a referral hospital in Kisumu County, Kenya; and to establish the role of co-infection and hormonal contraceptives on CIN.
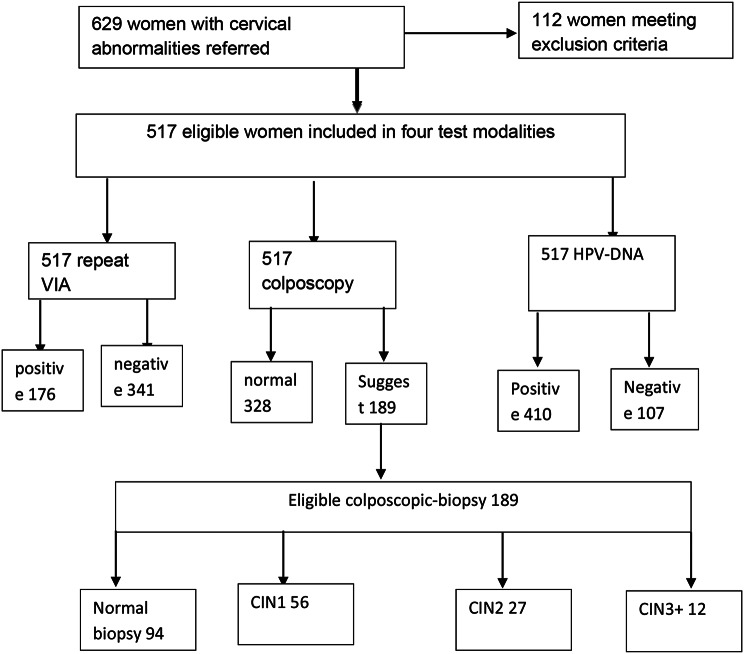
Method: In a cross-sectional study, we collected HPV, HIV, HSV-2 and CT data, cervical cytology results, and demographic information from 517 referrals. Blood samples were obtained for HIV and HSV-2 tests; urine for CT test, cervical swabs for hr-HPV test and colposcopic biopsy for histology confirmation after visual inspection with acetic acid (VIA).
Results: The overall prevalence of CIN was 18.4% (95/517) with CIN1 observed in 56(29.6%), CIN2 in 27(`14.3%), CIN3 and above (CIN3+) in 12(6.3%) and normal biopsy in 94(49.7%) of the patients out of which high grade CIN2 and above (CIN2+) was 7.54% (39/517) equivalent to 32.5 per 100,000 women per year. In a univariate analysis; HPV/HIV co-infection (infected vs. uninfected: OR 2.79; 95% CI 1.56-5.10, p < 0.001); HPV/HSV-2 co-infection (infected vs. uninfected: OR 2.41; 95% CI: 1.12-5.46, p < 0.024); HPV/CT co-infection (infected vs. uninfected: OR 3.83; 95% CI 1.84-8.51, p < 0.001) were found to be significantly associated with CIN. Additionally, hormone-containing intra uterine device (HIUD) contraceptives (users vs. none users: OR 1.43; 95% CI 0.28-10.9, p < 0.017) were also associated with CIN.
Conclusion: Co-infections with HIV, HSV-2 or Chlamydia trachomatis and use of HIUD were associated with increased risk of testing positive for CIN in HPV positive women. Although the overall prevalence of CIN was high, high-grade CIN2 + was comparable to the rates reported earlier. Therefore, population screening for co-infections alongside hr-HPV is desirable and is likely to reduce the burden of CIN in the region. Besides, women positive for hr-HPV and opting for contraceptives ought to be counseled about the possible positive and negative side-effects of different contraception options.
期刊介绍:
Infectious Agents and Cancer is an open access, peer-reviewed online journal that encompasses all aspects of basic, clinical, epidemiological and translational research providing an insight into the association between chronic infections and cancer.
The journal welcomes submissions in the pathogen-related cancer areas and other related topics, in particular:
• HPV and anogenital cancers, as well as head and neck cancers;
• EBV and Burkitt lymphoma;
• HCV/HBV and hepatocellular carcinoma as well as lymphoproliferative diseases;
• HHV8 and Kaposi sarcoma;
• HTLV and leukemia;
• Cancers in Low- and Middle-income countries.
The link between infection and cancer has become well established over the past 50 years, and infection-associated cancer contribute up to 16% of cancers in developed countries and 33% in less developed countries.
Preventive vaccines have been developed for only two cancer-causing viruses, highlighting both the opportunity to prevent infection-associated cancers by vaccination and the gaps that remain before vaccines can be developed for other cancer-causing agents. These gaps are due to incomplete understanding of the basic biology, natural history, epidemiology of many of the pathogens that cause cancer, the mechanisms they exploit to cause cancer, and how to interrupt progression to cancer in human populations. Early diagnosis or identification of lesions at high risk of progression represent the current most critical research area of the field supported by recent advances in genomics and proteomics technologies.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
