{"title":"The Feasibility of Early Shunting for Hydrocephalus after Subarachnoid Hemorrhage.","authors":"Naoki Nishizawa, Tomohiko Ozaki, Tomoki Kidani, Nobuyuki Izutsu, Shin Nakajima, Yonehiro Kanemura, Toshiyuki Fujinaka","doi":"10.2176/jns-nmc.2023-0300","DOIUrl":null,"url":null,"abstract":"<p><p>The feasibility of early shunting for hydrocephalus after the occurrence of subarachnoid hemorrhage has not yet been explored. We investigated factors associated with the development of hydrocephalus and the risk of shunt obstruction or infection in patients undergoing early shunt surgery. All cases of hydrocephalus after subarachnoid hemorrhage managed at our institution between January 2010 and December 2020 were included. Patients were classified based on the timing of shunt implantation after hemorrhage onset into either the early shunt group (≤28 days) or the late shunt group (>28 days). Of 138 subarachnoid hemorrhage patients managed during the recruitment period, 53 underwent shunt surgery, with 15 in the early shunt group and 38 in the late shunt group. The severity of subarachnoid hemorrhage, presence of Sylvian hematoma, and placement of an external ventricular and/or cisternal drain were significantly associated with the development of hydrocephalus. There was no significant difference between the early and late groups in terms of the rate of shunt obstruction or infection. In the early group, preoperative cerebrospinal fluid cell count was significantly higher in those who developed obstruction than those who did not (307.3 ± 238.2/3 μL vs. 73.8 ± 95.7/3 μL; p = 0.0364). This retrospective study showed no significant difference between early and late shunt implantation in the rate of shunt obstruction and infection. These findings suggests that planning shunt surgery in the early phase after subarachnoid hemorrhage might be feasible, depending on cerebrospinal fluid test results.</p>","PeriodicalId":19225,"journal":{"name":"Neurologia medico-chirurgica","volume":" ","pages":"177-185"},"PeriodicalIF":2.3000,"publicationDate":"2025-04-15","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12061559/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurologia medico-chirurgica","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.2176/jns-nmc.2023-0300","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/22 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
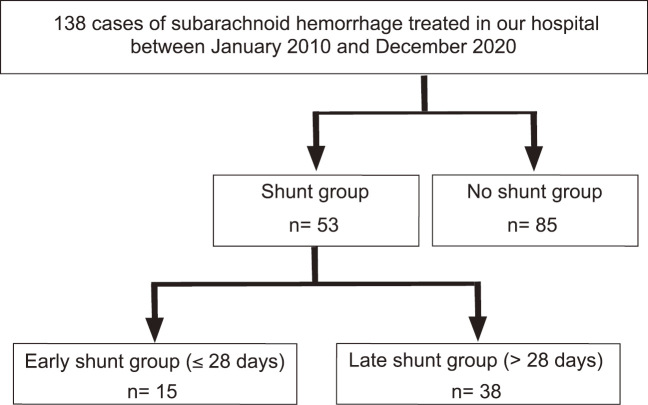
The feasibility of early shunting for hydrocephalus after the occurrence of subarachnoid hemorrhage has not yet been explored. We investigated factors associated with the development of hydrocephalus and the risk of shunt obstruction or infection in patients undergoing early shunt surgery. All cases of hydrocephalus after subarachnoid hemorrhage managed at our institution between January 2010 and December 2020 were included. Patients were classified based on the timing of shunt implantation after hemorrhage onset into either the early shunt group (≤28 days) or the late shunt group (>28 days). Of 138 subarachnoid hemorrhage patients managed during the recruitment period, 53 underwent shunt surgery, with 15 in the early shunt group and 38 in the late shunt group. The severity of subarachnoid hemorrhage, presence of Sylvian hematoma, and placement of an external ventricular and/or cisternal drain were significantly associated with the development of hydrocephalus. There was no significant difference between the early and late groups in terms of the rate of shunt obstruction or infection. In the early group, preoperative cerebrospinal fluid cell count was significantly higher in those who developed obstruction than those who did not (307.3 ± 238.2/3 μL vs. 73.8 ± 95.7/3 μL; p = 0.0364). This retrospective study showed no significant difference between early and late shunt implantation in the rate of shunt obstruction and infection. These findings suggests that planning shunt surgery in the early phase after subarachnoid hemorrhage might be feasible, depending on cerebrospinal fluid test results.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
