Damian Palus, Martyna Gołębiewska, Olga Piątek-Dalewska, Krzysztof Grudziński, Krzysztof Kuziemski, Radosław Owczuk, Michał Hoffmann, Dariusz Kozłowski, Tomasz Stefaniak
{"title":"Association of pre-existing comorbidities and complications with inpatient COVID-19 mortality - a single-center retrospective study.","authors":"Damian Palus, Martyna Gołębiewska, Olga Piątek-Dalewska, Krzysztof Grudziński, Krzysztof Kuziemski, Radosław Owczuk, Michał Hoffmann, Dariusz Kozłowski, Tomasz Stefaniak","doi":"10.5603/cj.103122","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>This study evaluates the impact of pre-existing comorbidities and in-hospital complications on COVID-19 mortality rates.</p><p><strong>Methods: </strong>A retrospective single-center study was conducted using electronic health records from 640 COVID-19 patients hospitalized at the University Clinical Centre in Gdansk, Poland, between November 2020 and May 2021. Patients were categorized based on disease severity into stable or ICU wards based on the disease severity. Data on demographics, comorbidities, complications, and treatments were collected and verified. Statistical analyses, including odds ratios (ORs) and confidence intervals (CIs), assessed mortality risk factors supported by python-based processing.</p><p><strong>Results: </strong>The mean patient age was 67 years (SD ± 15.89), comprising 39% females (n = 250) and 60.94% males (n = 390). Mortality risk was highest in patients aged 65 years and older (OR 3.00; 95% CI, 1.97-4.60). Among the pre-existing comorbidities, chronic kidney disease (OR 3.28; 95% CI, 2.12-5.09), atrial fibrillation (OR 2.43; CI 95%, 1.63-3.61), and heart failure (OR 2.89; 95% CI, 1.91-4.37) were significant predictors of mortality. In hospital complications, such as severe respiratory failure requiring ICU ventilation (OR 23.59; 95% CI, 2.81-197.87), myocardial infarction (OR 25.43; 95% CI, 3.16-204.97), acute kidney injury requiring renal replacement therapy (OR 19.15; 95% CI, 6.49-56.51), sepsis (OR 7.22, 95% CI, 3.77-13.84), stroke, further increased mortality risk.</p><p><strong>Conclusions: </strong>COVID-19 patients with pre-existing renal and cardiovascular conditions face a higher risk of fatal outcomes. Early diagnosis and intervention targeting these complications are vital to in reducing mortality. Further research is needed to reconcile disparities with existing literature.</p>","PeriodicalId":93923,"journal":{"name":"Cardiology journal","volume":" ","pages":"120-129"},"PeriodicalIF":0.0000,"publicationDate":"2025-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12068236/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cardiology journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5603/cj.103122","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/2/25 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
引用次数: 0
Abstract
Background: This study evaluates the impact of pre-existing comorbidities and in-hospital complications on COVID-19 mortality rates.
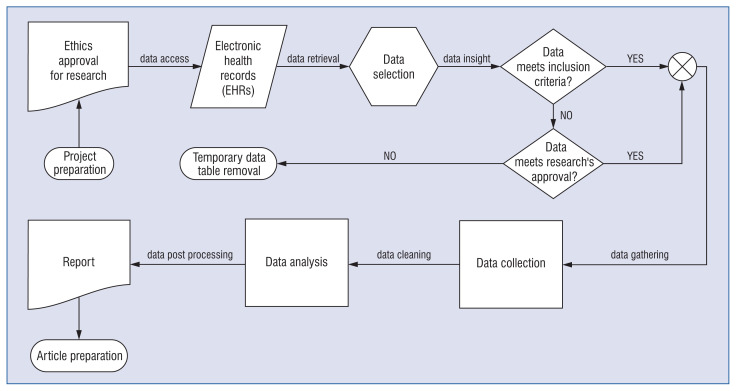
Methods: A retrospective single-center study was conducted using electronic health records from 640 COVID-19 patients hospitalized at the University Clinical Centre in Gdansk, Poland, between November 2020 and May 2021. Patients were categorized based on disease severity into stable or ICU wards based on the disease severity. Data on demographics, comorbidities, complications, and treatments were collected and verified. Statistical analyses, including odds ratios (ORs) and confidence intervals (CIs), assessed mortality risk factors supported by python-based processing.
Results: The mean patient age was 67 years (SD ± 15.89), comprising 39% females (n = 250) and 60.94% males (n = 390). Mortality risk was highest in patients aged 65 years and older (OR 3.00; 95% CI, 1.97-4.60). Among the pre-existing comorbidities, chronic kidney disease (OR 3.28; 95% CI, 2.12-5.09), atrial fibrillation (OR 2.43; CI 95%, 1.63-3.61), and heart failure (OR 2.89; 95% CI, 1.91-4.37) were significant predictors of mortality. In hospital complications, such as severe respiratory failure requiring ICU ventilation (OR 23.59; 95% CI, 2.81-197.87), myocardial infarction (OR 25.43; 95% CI, 3.16-204.97), acute kidney injury requiring renal replacement therapy (OR 19.15; 95% CI, 6.49-56.51), sepsis (OR 7.22, 95% CI, 3.77-13.84), stroke, further increased mortality risk.
Conclusions: COVID-19 patients with pre-existing renal and cardiovascular conditions face a higher risk of fatal outcomes. Early diagnosis and intervention targeting these complications are vital to in reducing mortality. Further research is needed to reconcile disparities with existing literature.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
