Objectives: Ultrasound-derived estimates of fetal size play an integral role in the prenatal management of twin pregnancy. These biometric measurements are conventionally plotted against singleton standards. We sought to establish fetal growth references for abdominal circumference, head circumference, biparietal diameter, femur diaphysis length and estimated fetal weight (EFW) in twin pregnancy. We also aimed to determine whether the performance of a twin fetal growth reference was superior to a singleton reference in the prediction of adverse perinatal outcome in twin pregnancies.
Methods: This was a retrospective analysis of data collected prospectively in the Evaluation of Sonographic Predictors of Restricted growth in Twins (ESPRiT) study, which was conducted at eight academic perinatal centers in Ireland, all with tertiary neonatal intensive care facilities. Only diamniotic twin pregnancies with two live fetuses were eligible for inclusion. Exclusion criteria were monoamnionicity, congenital abnormality, twin-to-twin transfusion syndrome or previable fetal demise (< 24 weeks' gestation). Using serial ultrasound observations, we applied fractional polynomial multilevel models to derive an equation for fetal centile determination. We compared these centiles with published singleton and twin fetal references, with particular focus on the Fetal Medicine Foundation (FMF) references. Using the last ultrasound examinations before delivery, we determined associations between biometric measures and a composite measure of adverse perinatal outcome (intraventricular hemorrhage, periventricular leukomalacia, hypoxic ischemic encephalopathy, necrotizing enterocolitis, bronchopulmonary dysplasia, sepsis or perinatal death), neonatal intensive care unit admission, preterm delivery (< 34 weeks) and birth-weight discordance ≥ 25%, based on the varied prevalence of these outcomes. We compared our results with the singleton and twin FMF reference ranges and the twin reference of the Southwest Thames Obstetric Research Collaborative (STORK) study.
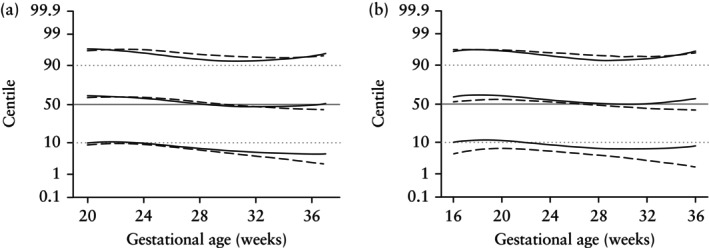
Results: Among the 948 twin pairs that met the inclusion criteria, 776 (81.9%) dichorionic and 172 (18.1%) monochorionic twin pairs completed the prospective 2-weekly ultrasound surveillance program. Fetal biometric measurements were obtained in 15 274 ultrasound assessments (12 279 in dichorionic and 2995 in monochorionic twin pairs) from serial ultrasound assessments. The median number of ultrasound assessments per pregnancy was 8 (interquartile range, 7-9). Growth trajectories in this cohort were consistent with the FMF and STORK published twin cohorts and notably less consistent with the FMF singleton standard. Compared with the FMF singleton standards, the 50th centiles for twins were greater early in pregnancy and lower later in pregnancy for all biometric measures, in both dichorionic and monochorionic twin pregnancies. This crossover in growth occurred at approximately 28 weeks' gestation for dichorionic twins and earlier for monochorionic twins. The 50th centiles for EFW were comparable to the FMF twin standards for both monochorionic and dichorionic twins, but with lower 10th centiles for dichorionic twins in the third trimester. The current (ESPRiT) twin reference ranges, the STORK twin reference ranges and the FMF twin reference ranges showed larger and statistically significant (P < 0.01) odds ratios for multiple biometric measures and multiple adverse perinatal outcomes, for both monochorionic and dichorionic twins, not observed with the FMF singleton reference standard.
期刊介绍:
Ultrasound in Obstetrics & Gynecology (UOG) is the official journal of the International Society of Ultrasound in Obstetrics and Gynecology (ISUOG) and is considered the foremost international peer-reviewed journal in the field. It publishes cutting-edge research that is highly relevant to clinical practice, which includes guidelines, expert commentaries, consensus statements, original articles, and systematic reviews. UOG is widely recognized and included in prominent abstract and indexing databases such as Index Medicus and Current Contents.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
