Lavanya Bathini, Nivethika Jeyakumar, Jessica Sontrop, Eric McArthur, Yuguang Kang, Bin Luo, Aminu Bello, David Collister, Sofia Ahmed, Padma Kaul, Erik Youngson, Branko Braam, Nir Melamed, Michelle Hladunewich, Amit X Garg
{"title":"Impact of Baseline Kidney Function on the Rate of Progressive Kidney Disease After Pregnancy: A Population-Based Cohort Study Research Protocol.","authors":"Lavanya Bathini, Nivethika Jeyakumar, Jessica Sontrop, Eric McArthur, Yuguang Kang, Bin Luo, Aminu Bello, David Collister, Sofia Ahmed, Padma Kaul, Erik Youngson, Branko Braam, Nir Melamed, Michelle Hladunewich, Amit X Garg","doi":"10.1177/20543581251318836","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Better data are necessary to determine whether baseline level of kidney function affects the rate of progressive kidney disease following pregnancy.</p><p><strong>Objective: </strong>The objective was to determine whether the baseline (pre-pregnancy) estimated glomerular filtration rate (eGFR) modifies the association between becoming pregnant and the subsequent rate of progressive kidney disease.</p><p><strong>Design: </strong>Population-based cohort study using provincial administrative health care databases in Ontario and Alberta, Canada.</p><p><strong>Setting: </strong>The sample will be accrued from April 1, 2007, to March 31, 2023, in Ontario and from April 1, 2012, to March 31, 2023, in Alberta. Follow-up for study outcomes will occur until March 31, 2024.</p><p><strong>Participants: </strong>The pregnant group will include adult female residents of Ontario or Alberta with a record of a pregnancy of 20 to 46 weeks' gestation during the accrual period, and the non-pregnant group will include adult female residents with no prior record of pregnancy. The cohort entry dates in those in the pregnant group will be the estimated date of conception; the entry dates for those in the non-pregnant group will be randomly assigned following the distribution of dates in the pregnant group. To be eligible, individuals must be between 18 and 45 years old at cohort entry. They require at least 1 serum creatinine measurement within 2 years before entry and should not have received maintenance dialysis or a prior kidney transplant. Both groups will be categorized into one of 3 levels of baseline eGFR (≥60, 45-59, and <45 mL/min per 1.73 m<sup>2</sup>). Inverse probability of treatment weighting on a propensity score will be used to balance the pregnant and non-pregnant groups on baseline characteristics (including age, proteinuria, hypertension, and diabetes) within the 3 categories of baseline eGFR.</p><p><strong>Measurements: </strong>The primary outcome, progressive kidney disease, will be defined as a composite of a persistent ≥40% drop in eGFR from the baseline value, a new persistent eGFR <15 mL/min per 1.73 m<sup>2</sup>, receipt of maintenance dialysis, or receipt of a kidney transplant. The secondary outcomes will be the components of the primary composite outcome examined separately and the annualized change in eGFR in mL/min per 1.73 m<sup>2</sup> from baseline.</p><p><strong>Methods: </strong>We will test for statistical interaction to determine whether the baseline category of eGFR modifies the rate of long-term progressive kidney disease after pregnancy. We hypothesize that a statistical interaction will be present. We will present weighted cause-specific hazard ratios (HRs) and cumulative incidence function (CIF) curves for up to 10 years of follow-up for the pregnant and non-pregnant groups stratified by each eGFR category. We will perform additional pre-specified analyses to confirm whether the findings are robust and examine associations that account for baseline proteinuria.</p><p><strong>Results: </strong>Based on a feasibility analysis using ICES data in Ontario, we expect the cohort to include over 400 000 pregnant females and 1.2 million non-pregnant females. This includes at least 395 000 pregnant females with baseline eGFR ≥60 mL/min/1.73 m<sup>2</sup>, 300 with eGFR 45 to 59 mL/min/1.73 m<sup>2</sup>, and 110 with eGFR <45 mL/min/1.73 m<sup>2</sup>. The median follow-up is anticipated to be 5 years (range = 1-17 years) with minimal loss to follow-up.</p><p><strong>Limitations: </strong>Measures of kidney function will be obtained as part of routine care (not according to a research schedule). Measures of baseline proteinuria are frequently missing from routine care data, even in up to 15% of those with an eGFR <45 mL/min per 1.73 m<sup>2</sup>.</p><p><strong>Conclusion: </strong>This study will investigate whether the level of baseline eGFR modifies the rate of progressive kidney disease after pregnancy and will estimate the cumulative incidence of progressive kidney disease in pregnant and non-pregnant females across 3 categories of baseline eGFR.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"12 ","pages":"20543581251318836"},"PeriodicalIF":1.5000,"publicationDate":"2025-02-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11869263/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581251318836","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Better data are necessary to determine whether baseline level of kidney function affects the rate of progressive kidney disease following pregnancy.
Objective: The objective was to determine whether the baseline (pre-pregnancy) estimated glomerular filtration rate (eGFR) modifies the association between becoming pregnant and the subsequent rate of progressive kidney disease.
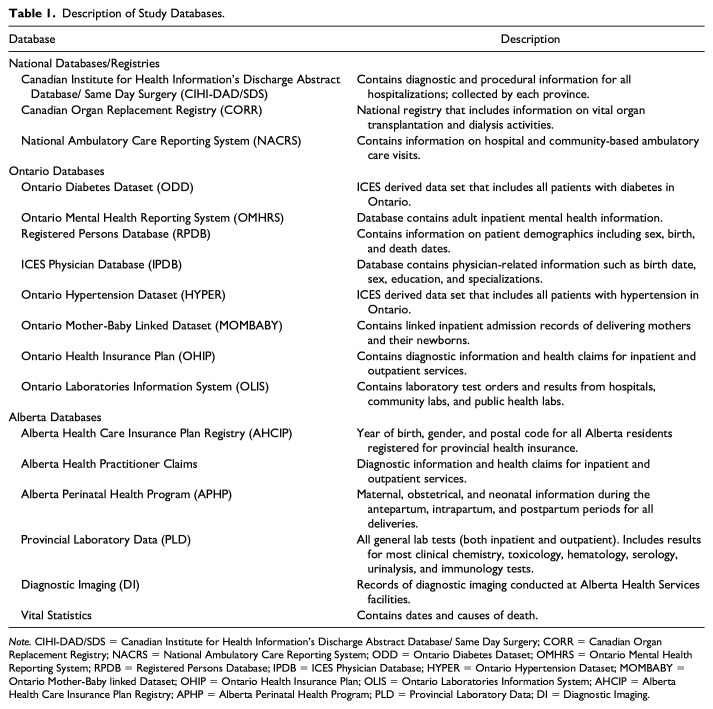
Design: Population-based cohort study using provincial administrative health care databases in Ontario and Alberta, Canada.
Setting: The sample will be accrued from April 1, 2007, to March 31, 2023, in Ontario and from April 1, 2012, to March 31, 2023, in Alberta. Follow-up for study outcomes will occur until March 31, 2024.
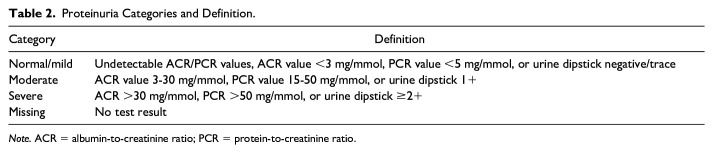
Participants: The pregnant group will include adult female residents of Ontario or Alberta with a record of a pregnancy of 20 to 46 weeks' gestation during the accrual period, and the non-pregnant group will include adult female residents with no prior record of pregnancy. The cohort entry dates in those in the pregnant group will be the estimated date of conception; the entry dates for those in the non-pregnant group will be randomly assigned following the distribution of dates in the pregnant group. To be eligible, individuals must be between 18 and 45 years old at cohort entry. They require at least 1 serum creatinine measurement within 2 years before entry and should not have received maintenance dialysis or a prior kidney transplant. Both groups will be categorized into one of 3 levels of baseline eGFR (≥60, 45-59, and <45 mL/min per 1.73 m2). Inverse probability of treatment weighting on a propensity score will be used to balance the pregnant and non-pregnant groups on baseline characteristics (including age, proteinuria, hypertension, and diabetes) within the 3 categories of baseline eGFR.
Measurements: The primary outcome, progressive kidney disease, will be defined as a composite of a persistent ≥40% drop in eGFR from the baseline value, a new persistent eGFR <15 mL/min per 1.73 m2, receipt of maintenance dialysis, or receipt of a kidney transplant. The secondary outcomes will be the components of the primary composite outcome examined separately and the annualized change in eGFR in mL/min per 1.73 m2 from baseline.
Methods: We will test for statistical interaction to determine whether the baseline category of eGFR modifies the rate of long-term progressive kidney disease after pregnancy. We hypothesize that a statistical interaction will be present. We will present weighted cause-specific hazard ratios (HRs) and cumulative incidence function (CIF) curves for up to 10 years of follow-up for the pregnant and non-pregnant groups stratified by each eGFR category. We will perform additional pre-specified analyses to confirm whether the findings are robust and examine associations that account for baseline proteinuria.
Results: Based on a feasibility analysis using ICES data in Ontario, we expect the cohort to include over 400 000 pregnant females and 1.2 million non-pregnant females. This includes at least 395 000 pregnant females with baseline eGFR ≥60 mL/min/1.73 m2, 300 with eGFR 45 to 59 mL/min/1.73 m2, and 110 with eGFR <45 mL/min/1.73 m2. The median follow-up is anticipated to be 5 years (range = 1-17 years) with minimal loss to follow-up.
Limitations: Measures of kidney function will be obtained as part of routine care (not according to a research schedule). Measures of baseline proteinuria are frequently missing from routine care data, even in up to 15% of those with an eGFR <45 mL/min per 1.73 m2.
Conclusion: This study will investigate whether the level of baseline eGFR modifies the rate of progressive kidney disease after pregnancy and will estimate the cumulative incidence of progressive kidney disease in pregnant and non-pregnant females across 3 categories of baseline eGFR.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
