{"title":"Clinical outcomes in patients with cardiorenal multimorbidity: the role of serum uric acid/serum creatinine ratio.","authors":"Antonietta Gigante, Eleonora Assanto, Claudia Brigato, Chiara Pellicano, Francesco Iannazzo, Edoardo Rosato, Maurizio Muscaritoli, Claudio Ferri, Rosario Cianci","doi":"10.1007/s40292-025-00706-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Serum uric acid (SUA), the final product of purine metabolism, is an independent risk factor for cardiovascular (CV) disease. Since SUA levels depend on renal function, SUA to serum creatinine ratio (SUA/sCr) is emerging as a more specific biomarker of CV risk.</p><p><strong>Aim: </strong>To evaluate in hospitalized patients with cardiorenal multimorbidity (CRM) if the SUA/sCr ≥ 5.35 is associated with clinical outcomes. The primary outcome was in-hospital mortality. The secondary outcome was the composite of all-cause of mortality and adverse clinical events.</p><p><strong>Methods: </strong>We conducted a retrospective review of medical records from consecutive CRM inpatients admitted to the medical ward. The composite endpoint was calculated as all-cause mortality and adverse clinical events such as acute coronary syndrome, stroke, infections, and renal replacement therapy.</p><p><strong>Results: </strong>In our cohort, 141 patients (mean age of 75.6 ± 10.2 years) were identified with CRM. In-hospital mortality occurred in 17 patients (16%), and 64 patients (60.4%) experienced adverse clinical outcomes. Among the 106 patients, 20 (18.9%) had an SUA/sCr ≥ 5.35, while 86 (81.1%) had an SUA/sCr < 5.35. Male gender was significantly associated with SUA/sCr ≥ 5.35 (p = 0.007). In-hospital mortality was significantly higher in patients with SUA/sCr ≥ 5.35 (p = 0.010), and a positive correlation with adverse clinical outcomes was documented in this subgroup (p = 0.012).</p><p><strong>Conclusion: </strong>in patients with CRM, SUA/sCr ≥ 5.35 is associated with increased in-hospital mortality and worse clinical outcomes. The ratio and related cut-off value of SUA/sCr could represent a useful biomarker to assess in-hospital complications in CRM patients.</p>","PeriodicalId":12890,"journal":{"name":"High Blood Pressure & Cardiovascular Prevention","volume":" ","pages":"209-216"},"PeriodicalIF":2.9000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11890324/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"High Blood Pressure & Cardiovascular Prevention","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40292-025-00706-z","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/4 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
引用次数: 0
Abstract
Introduction: Serum uric acid (SUA), the final product of purine metabolism, is an independent risk factor for cardiovascular (CV) disease. Since SUA levels depend on renal function, SUA to serum creatinine ratio (SUA/sCr) is emerging as a more specific biomarker of CV risk.
Aim: To evaluate in hospitalized patients with cardiorenal multimorbidity (CRM) if the SUA/sCr ≥ 5.35 is associated with clinical outcomes. The primary outcome was in-hospital mortality. The secondary outcome was the composite of all-cause of mortality and adverse clinical events.
Methods: We conducted a retrospective review of medical records from consecutive CRM inpatients admitted to the medical ward. The composite endpoint was calculated as all-cause mortality and adverse clinical events such as acute coronary syndrome, stroke, infections, and renal replacement therapy.
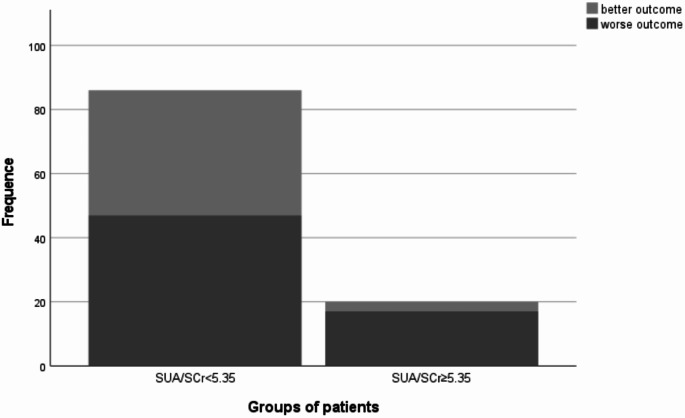
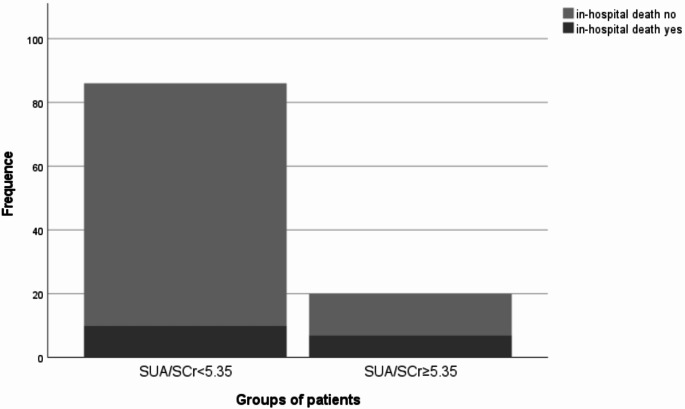
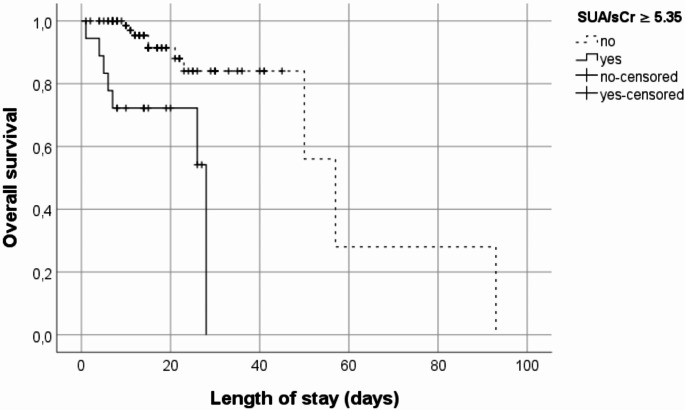
Results: In our cohort, 141 patients (mean age of 75.6 ± 10.2 years) were identified with CRM. In-hospital mortality occurred in 17 patients (16%), and 64 patients (60.4%) experienced adverse clinical outcomes. Among the 106 patients, 20 (18.9%) had an SUA/sCr ≥ 5.35, while 86 (81.1%) had an SUA/sCr < 5.35. Male gender was significantly associated with SUA/sCr ≥ 5.35 (p = 0.007). In-hospital mortality was significantly higher in patients with SUA/sCr ≥ 5.35 (p = 0.010), and a positive correlation with adverse clinical outcomes was documented in this subgroup (p = 0.012).
Conclusion: in patients with CRM, SUA/sCr ≥ 5.35 is associated with increased in-hospital mortality and worse clinical outcomes. The ratio and related cut-off value of SUA/sCr could represent a useful biomarker to assess in-hospital complications in CRM patients.
期刊介绍:
High Blood Pressure & Cardiovascular Prevention promotes knowledge, update and discussion in the field of hypertension and cardiovascular disease prevention, by providing a regular programme of independent review articles covering key aspects of the management of hypertension and cardiovascular diseases. The journal includes: Invited ''State of the Art'' reviews. Expert commentaries on guidelines, major trials, technical advances.Presentation of new intervention trials design.''Pros and Cons'' or round tables on controversial issues.Statements on guidelines from hypertension and cardiovascular scientific societies.Socio-economic issues.Cost/benefit in prevention of cardiovascular diseases.Monitoring of healthcare systems.News and views from the Italian Society of Hypertension (including abstracts).All manuscripts are subject to peer review by international experts. Letters to the editor are welcomed and will be considered for publication.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
