Treatment Patterns, Adverse Events, and Clinical Outcomes with Steroidal Mineralocorticoid Receptor Antagonists: A Retrospective Analysis of Administrative Claims Data (RELICS).
Emma L Richard, Nihar R Desai, Vincent J Willey, Alain Gay, Charlie Scott, Kerstin Folkerts, Elena Pessina, Rakesh Singh, Chia-Chen Teng, Nikolaus G Oberprieler
{"title":"Treatment Patterns, Adverse Events, and Clinical Outcomes with Steroidal Mineralocorticoid Receptor Antagonists: A Retrospective Analysis of Administrative Claims Data (RELICS).","authors":"Emma L Richard, Nihar R Desai, Vincent J Willey, Alain Gay, Charlie Scott, Kerstin Folkerts, Elena Pessina, Rakesh Singh, Chia-Chen Teng, Nikolaus G Oberprieler","doi":"10.2147/POR.S489791","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to describe the characteristics, treatment patterns, adverse events (AEs), and clinical outcomes of patients starting steroidal mineralocorticoid receptor antagonists (sMRAs) in real-world settings.</p><p><strong>Methods: </strong>The RELICS study, complementing the survey-based RELICS-PS study, was a retrospective cohort study conducted using the Healthcare Integrated Research Database (HIRD<sup>®</sup>), a single-payer healthcare database with medical and pharmacy claims from health insurance plans across the United States. A cohort of adults initiating sMRAs from January 2016 to June 2021 was divided into six subgroups: three mutually exclusive heart failure (HF) subgroups, two mutually exclusive chronic kidney disease (CKD) subgroups, and \"all other patients\" subgroup, which included those without documented HF or CKD. Outcomes assessed from the first sMRA fill until death, health-plan disenrollment, or June 2022 (whichever came first) included analysis of treatment patterns, AEs, and clinical outcomes. Factors associated with sMRA discontinuation were evaluated with multivariate logistic regression.</p><p><strong>Results: </strong>Of the 224,100 sMRA initiators identified, 76.4% did not have documented HF or CKD (ie, \"all other patients\" subgroup). This subgroup was younger and primarily female. Across all initiators, 72.3% were nonadherent, and 73.0% discontinued treatment within a median of 90 days of initiation. Of these discontinuers, 44.2% restarted treatment within a median of 91 days of discontinuation. Factors decreasing odds of discontinuation across most subgroups included a higher comorbidity burden, use of other cardiovascular medications, and cardiologist prescribing. These findings were consistent across subgroups. AEs and clinical outcomes varied across subgroups in line with baseline comorbidity profiles. Patients with a higher comorbidity burden, such as those with both CKD and T2D rather than CKD alone, experienced worse outcomes.</p><p><strong>Conclusion: </strong>High rates of treatment discontinuation and subsequent restart were observed across all subgroups, implying fluctuating sMRA use. However, heightened cardiovascular risk may decrease the odds of discontinuation.</p>","PeriodicalId":20399,"journal":{"name":"Pragmatic and Observational Research","volume":"16 ","pages":"27-37"},"PeriodicalIF":2.7000,"publicationDate":"2025-02-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11873017/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pragmatic and Observational Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.2147/POR.S489791","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: This study aimed to describe the characteristics, treatment patterns, adverse events (AEs), and clinical outcomes of patients starting steroidal mineralocorticoid receptor antagonists (sMRAs) in real-world settings.
Methods: The RELICS study, complementing the survey-based RELICS-PS study, was a retrospective cohort study conducted using the Healthcare Integrated Research Database (HIRD®), a single-payer healthcare database with medical and pharmacy claims from health insurance plans across the United States. A cohort of adults initiating sMRAs from January 2016 to June 2021 was divided into six subgroups: three mutually exclusive heart failure (HF) subgroups, two mutually exclusive chronic kidney disease (CKD) subgroups, and "all other patients" subgroup, which included those without documented HF or CKD. Outcomes assessed from the first sMRA fill until death, health-plan disenrollment, or June 2022 (whichever came first) included analysis of treatment patterns, AEs, and clinical outcomes. Factors associated with sMRA discontinuation were evaluated with multivariate logistic regression.
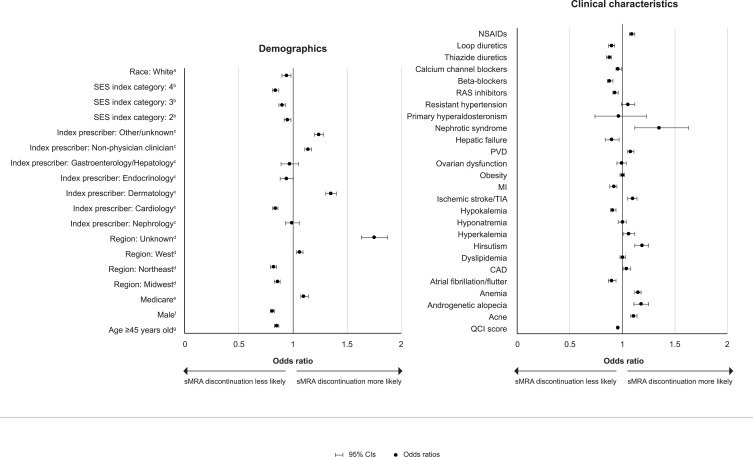
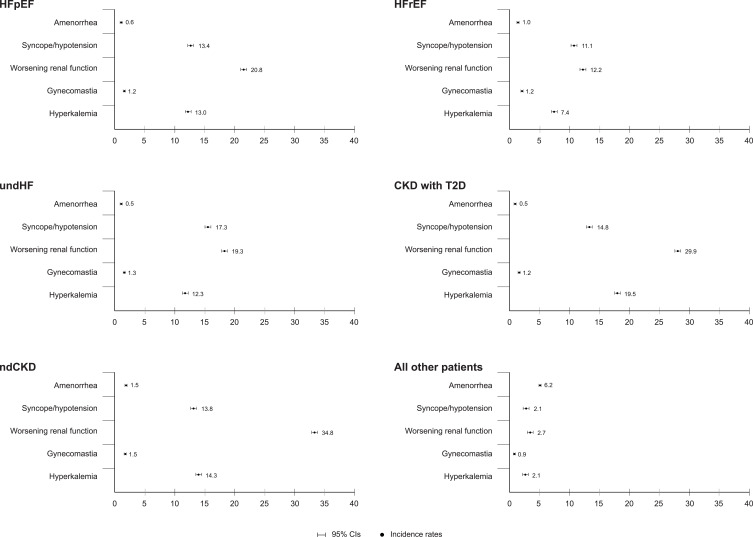
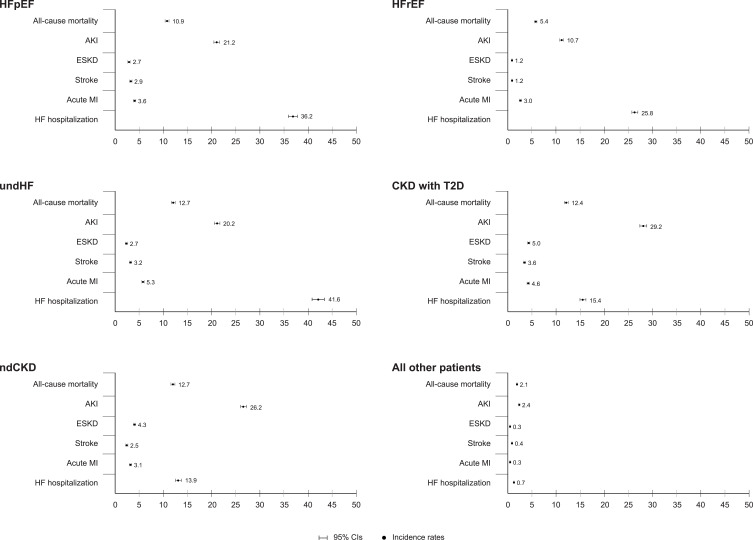
Results: Of the 224,100 sMRA initiators identified, 76.4% did not have documented HF or CKD (ie, "all other patients" subgroup). This subgroup was younger and primarily female. Across all initiators, 72.3% were nonadherent, and 73.0% discontinued treatment within a median of 90 days of initiation. Of these discontinuers, 44.2% restarted treatment within a median of 91 days of discontinuation. Factors decreasing odds of discontinuation across most subgroups included a higher comorbidity burden, use of other cardiovascular medications, and cardiologist prescribing. These findings were consistent across subgroups. AEs and clinical outcomes varied across subgroups in line with baseline comorbidity profiles. Patients with a higher comorbidity burden, such as those with both CKD and T2D rather than CKD alone, experienced worse outcomes.
Conclusion: High rates of treatment discontinuation and subsequent restart were observed across all subgroups, implying fluctuating sMRA use. However, heightened cardiovascular risk may decrease the odds of discontinuation.
期刊介绍:
Pragmatic and Observational Research is an international, peer-reviewed, open-access journal that publishes data from studies designed to closely reflect medical interventions in real-world clinical practice, providing insights beyond classical randomized controlled trials (RCTs). While RCTs maximize internal validity for cause-and-effect relationships, they often represent only specific patient groups. This journal aims to complement such studies by providing data that better mirrors real-world patients and the usage of medicines, thus informing guidelines and enhancing the applicability of research findings across diverse patient populations encountered in everyday clinical practice.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
