David Fellows, Julia Kotowska, Thomas Stevenson, Jennifer Brown, Zsolt Orosz, Ather Siddiqi, Duncan Whitwell, Thomas Cosker, Christopher L M H GIbbons
{"title":"Management and surveillance of metastatic giant cell tumour of bone.","authors":"David Fellows, Julia Kotowska, Thomas Stevenson, Jennifer Brown, Zsolt Orosz, Ather Siddiqi, Duncan Whitwell, Thomas Cosker, Christopher L M H GIbbons","doi":"10.3389/pore.2025.1611916","DOIUrl":null,"url":null,"abstract":"<p><p>Giant cell tumour of bone (GCTB) is viewed as a benign, locally aggressive primary bone tumour with metastatic potential. Current management is surgery with bone curettage or resection and systemic therapy with denosumab. Diagnosis is confirmed histologically prior to surgery, with staging for pulmonary disease, as pulmonary metastases (PM) reportedly occur in <8%. This study aimed to assess incidence, surveillance and management of PM in patients with GCTB, with histopathological review. A retrospective audit of the Oxford bone tumour registry was performed from January 2014 - October 2023. Inclusion criterion was histological confirmation of GCTB. Exclusion criteria were incomplete medical, imaging or histology records, or referral for secondary MDT opinion for diagnosis. From an initial group of 126 GCTB patients, 83 patients met the full selection criteria. Pulmonary metastases were identified in 11 patients. Three with PM were excluded on histopathological review as being giant cell rich osteosarcoma rather than metastatic GCTB. This left 8 (9.6%) patients, one had PM at presentation and seven at follow-up between 2 and 42 months. Two were histologically confirmed after cardiothoracic surgery and biopsy, six radiologically diagnosed. Three (37.5%) patients with PM have died (between 1 and 12 months after confirmed PM), five are alive with stable disease. Seven (87.5%) of patients with pulmonary disease were treated with denosumab/chemotherapy (three before, four after pulmonary diagnosis). Five (62.5%) with pulmonary disease had recurrence of local disease requiring further surgery. Local recurrence was an independent risk factor for PM on statistical analysis. GCTB may present with PM, but more commonly, metastasis occurs after surgery, presenting on surveillance and can progress. There were no distinct differences in histopathological appearance between patients with GCTB that developed PM and those that did not, therefore morphological features of the tumour cannot be currently used to predict tumour behaviour. PM can behave aggressively, necessitating identifying histological markers to recognise patients at risk of metastatic GCTB, for example, through mRNA single cell analysis. We propose GCTB patients with PM receive regular chest surveillance with PET scan and/or CT to monitor disease progression, and a multi-centre audit of GCTB outcome undertaken to further define optimal clinical management.</p>","PeriodicalId":19981,"journal":{"name":"Pathology & Oncology Research","volume":"31 ","pages":"1611916"},"PeriodicalIF":2.3000,"publicationDate":"2025-02-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11879744/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Pathology & Oncology Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.3389/pore.2025.1611916","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"ONCOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
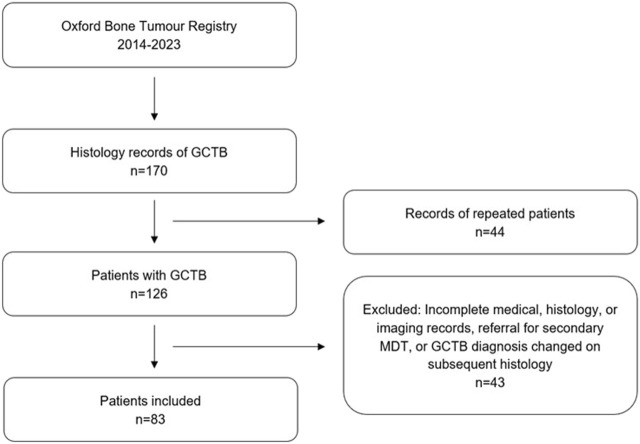
Giant cell tumour of bone (GCTB) is viewed as a benign, locally aggressive primary bone tumour with metastatic potential. Current management is surgery with bone curettage or resection and systemic therapy with denosumab. Diagnosis is confirmed histologically prior to surgery, with staging for pulmonary disease, as pulmonary metastases (PM) reportedly occur in <8%. This study aimed to assess incidence, surveillance and management of PM in patients with GCTB, with histopathological review. A retrospective audit of the Oxford bone tumour registry was performed from January 2014 - October 2023. Inclusion criterion was histological confirmation of GCTB. Exclusion criteria were incomplete medical, imaging or histology records, or referral for secondary MDT opinion for diagnosis. From an initial group of 126 GCTB patients, 83 patients met the full selection criteria. Pulmonary metastases were identified in 11 patients. Three with PM were excluded on histopathological review as being giant cell rich osteosarcoma rather than metastatic GCTB. This left 8 (9.6%) patients, one had PM at presentation and seven at follow-up between 2 and 42 months. Two were histologically confirmed after cardiothoracic surgery and biopsy, six radiologically diagnosed. Three (37.5%) patients with PM have died (between 1 and 12 months after confirmed PM), five are alive with stable disease. Seven (87.5%) of patients with pulmonary disease were treated with denosumab/chemotherapy (three before, four after pulmonary diagnosis). Five (62.5%) with pulmonary disease had recurrence of local disease requiring further surgery. Local recurrence was an independent risk factor for PM on statistical analysis. GCTB may present with PM, but more commonly, metastasis occurs after surgery, presenting on surveillance and can progress. There were no distinct differences in histopathological appearance between patients with GCTB that developed PM and those that did not, therefore morphological features of the tumour cannot be currently used to predict tumour behaviour. PM can behave aggressively, necessitating identifying histological markers to recognise patients at risk of metastatic GCTB, for example, through mRNA single cell analysis. We propose GCTB patients with PM receive regular chest surveillance with PET scan and/or CT to monitor disease progression, and a multi-centre audit of GCTB outcome undertaken to further define optimal clinical management.
期刊介绍:
Pathology & Oncology Research (POR) is an interdisciplinary Journal at the interface of pathology and oncology including the preclinical and translational research, diagnostics and therapy. Furthermore, POR is an international forum for the rapid communication of reviews, original research, critical and topical reports with excellence and novelty. Published quarterly, POR is dedicated to keeping scientists informed of developments on the selected biomedical fields bridging the gap between basic research and clinical medicine. It is a special aim for POR to promote pathological and oncological publishing activity of colleagues in the Central and East European region. The journal will be of interest to pathologists, and a broad range of experimental and clinical oncologists, and related experts. POR is supported by an acknowledged international advisory board and the Arányi Fundation for modern pathology.


 分享
分享

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
