Differences in the risk of frailty based on care receipt, unmet care needs and socio-economic inequalities: A longitudinal analysis of the English Longitudinal Study of Ageing.
David R Sinclair, Asri Maharani, Andrew Clegg, Barbara Hanratty, Gindo Tampubolon, Chris Todd, Raphael Wittenberg, Terence W O'Neill, Fiona E Matthews
{"title":"Differences in the risk of frailty based on care receipt, unmet care needs and socio-economic inequalities: A longitudinal analysis of the English Longitudinal Study of Ageing.","authors":"David R Sinclair, Asri Maharani, Andrew Clegg, Barbara Hanratty, Gindo Tampubolon, Chris Todd, Raphael Wittenberg, Terence W O'Neill, Fiona E Matthews","doi":"10.1016/j.tjfa.2025.100012","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The older population is increasingly reliant on social care, especially those who are frail. However, an estimated 1.5 million people over 65 in England have unmet care needs. The relationship between receiving care, or receiving insufficient care, and changes in frailty status remains unclear.</p><p><strong>Objectives: </strong>To investigate the associations between care receipt (paid or unpaid), unmet care needs, frailty status, and mortality.</p><p><strong>Design: </strong>We used multistate models to estimate the risk of increasing or decreasing levels of frailty, using English Longitudinal Study of Ageing (ELSA) data. Covariates included age, gender, wealth, area deprivation, education, and marital status. Care status was assessed through received care and self-reported unmet care needs, while frailty status was determined using a frailty index.</p><p><strong>Participants: </strong>15,003 individuals aged 50+, using data collected over 18 years (2002-2019).</p><p><strong>Results: </strong>Individuals who receive care are more susceptible to frailty and are less likely to recover from frailty to a less frail state. The hazard ratio of males receiving care transitioning from prefrailty to frailty was 2.1 [95 % CI: 1.7-2.6] and for females 1.8 [1.5-2.0]. Wealth is an equally influential predictor of changes in frailty status: individuals in the lowest wealth quintile who do not receive care are as likely to become frail as those in the highest wealth quintile who do receive care. As individuals receiving care (including unpaid care) are likely to be in poorer health than those who do not receive care, this highlights stark inequalities in the risk of frailty between the richest and poorest individuals. Unmet care needs were associated with transitioning from prefrailty to frailty for males (hazard ratio: 1.7 [1.2-2.4]) but not for females.</p><p><strong>Conclusions: </strong>Individuals starting to receive care (paid or unpaid) and people in the poorest wealth quintile are target groups for interventions aimed at delaying the onset of frailty.</p>","PeriodicalId":51629,"journal":{"name":"Journal of Frailty & Aging","volume":"14 2","pages":"100012"},"PeriodicalIF":3.3000,"publicationDate":"2025-04-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11959111/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Frailty & Aging","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1016/j.tjfa.2025.100012","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/3/7 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The older population is increasingly reliant on social care, especially those who are frail. However, an estimated 1.5 million people over 65 in England have unmet care needs. The relationship between receiving care, or receiving insufficient care, and changes in frailty status remains unclear.
Objectives: To investigate the associations between care receipt (paid or unpaid), unmet care needs, frailty status, and mortality.
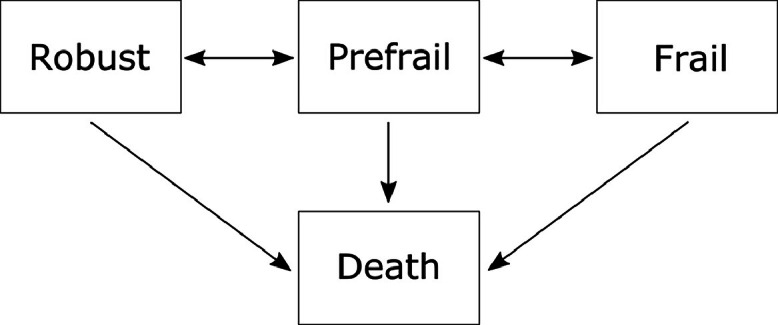
Design: We used multistate models to estimate the risk of increasing or decreasing levels of frailty, using English Longitudinal Study of Ageing (ELSA) data. Covariates included age, gender, wealth, area deprivation, education, and marital status. Care status was assessed through received care and self-reported unmet care needs, while frailty status was determined using a frailty index.
Participants: 15,003 individuals aged 50+, using data collected over 18 years (2002-2019).
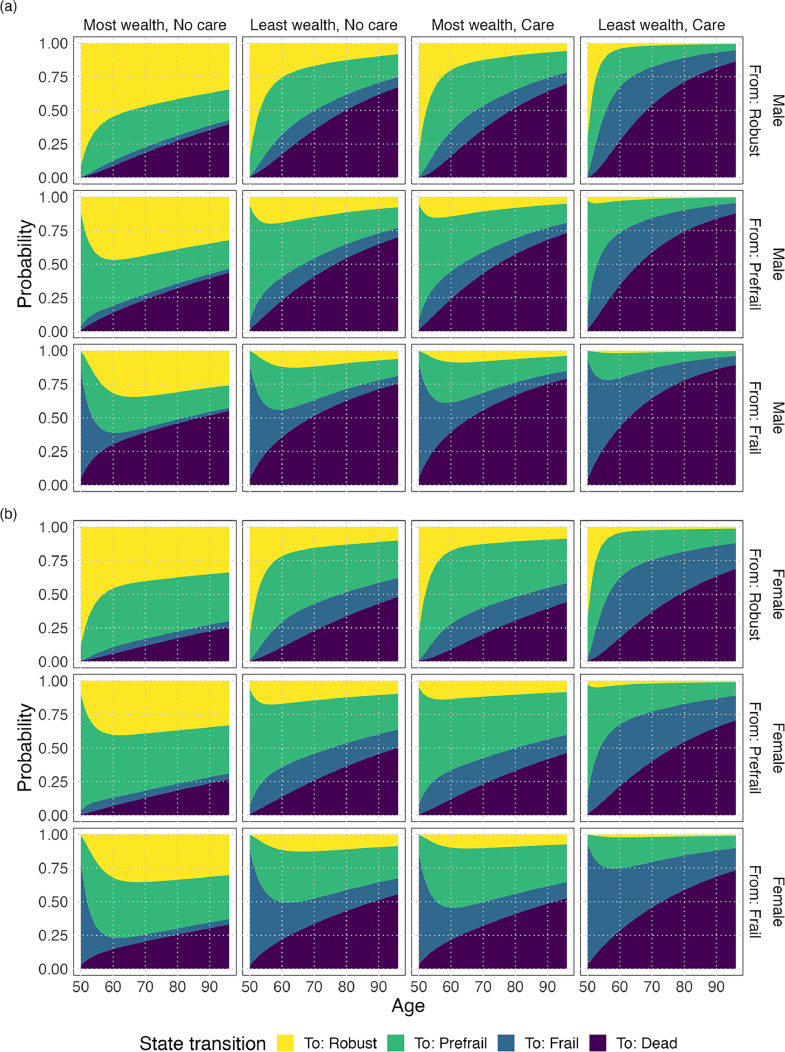
Results: Individuals who receive care are more susceptible to frailty and are less likely to recover from frailty to a less frail state. The hazard ratio of males receiving care transitioning from prefrailty to frailty was 2.1 [95 % CI: 1.7-2.6] and for females 1.8 [1.5-2.0]. Wealth is an equally influential predictor of changes in frailty status: individuals in the lowest wealth quintile who do not receive care are as likely to become frail as those in the highest wealth quintile who do receive care. As individuals receiving care (including unpaid care) are likely to be in poorer health than those who do not receive care, this highlights stark inequalities in the risk of frailty between the richest and poorest individuals. Unmet care needs were associated with transitioning from prefrailty to frailty for males (hazard ratio: 1.7 [1.2-2.4]) but not for females.
Conclusions: Individuals starting to receive care (paid or unpaid) and people in the poorest wealth quintile are target groups for interventions aimed at delaying the onset of frailty.
期刊介绍:
The Journal of Frailty & Aging is a peer-reviewed international journal aimed at presenting articles that are related to research in the area of aging and age-related (sub)clinical conditions. In particular, the journal publishes high-quality papers describing and discussing social, biological, and clinical features underlying the onset and development of frailty in older persons. The Journal of Frailty & Aging is composed by five different sections: - Biology of frailty and aging In this section, the journal presents reports from preclinical studies and experiences focused at identifying, describing, and understanding the subclinical pathophysiological mechanisms at the basis of frailty and aging. - Physical frailty and age-related body composition modifications Studies exploring the physical and functional components of frailty are contained in this section. Moreover, since body composition plays a major role in determining physical frailty and, at the same time, represents the most evident feature of the aging process, special attention is given to studies focused on sarcopenia and obesity at older age. - Neurosciences of frailty and aging The section presents results from studies exploring the cognitive and neurological aspects of frailty and age-related conditions. In particular, papers on neurodegenerative conditions of advanced age are welcomed. - Frailty and aging in clinical practice and public health This journal’s section is devoted at presenting studies on clinical issues of frailty and age-related conditions. This multidisciplinary section particularly welcomes reports from clinicians coming from different backgrounds and specialties dealing with the heterogeneous clinical manifestations of advanced age. Moreover, this part of the journal also contains reports on frailty- and age-related social and public health issues. - Clinical trials and therapeutics This final section contains all the manuscripts presenting data on (pharmacological and non-pharmacological) interventions aimed at preventing, delaying, or treating frailty and age-related conditions.The Journal of Frailty & Aging is a quarterly publication of original papers, review articles, case reports, controversies, letters to the Editor, and book reviews. Manuscripts will be evaluated by the editorial staff and, if suitable, by expert reviewers assigned by the editors. The journal particularly welcomes papers by researchers from different backgrounds and specialities who may want to share their views and experiences on the common themes of frailty and aging.The abstracting and indexing of the Journal of Frailty & Aging is covered by MEDLINE (approval by the National Library of Medicine in February 2016).



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
