To cut or not to cut? Extended mesenteric excision during intestinal resection does not impact the postoperative recurrence nor the postoperative complications in Crohn's disease: a systematic review and meta-analysis.
M Topala, P Martinekova, A Rancz, D S Veres, K Lenti, P Miheller, B Erőss, P Hegyi, S Ábrahám
{"title":"To cut or not to cut? Extended mesenteric excision during intestinal resection does not impact the postoperative recurrence nor the postoperative complications in Crohn's disease: a systematic review and meta-analysis.","authors":"M Topala, P Martinekova, A Rancz, D S Veres, K Lenti, P Miheller, B Erőss, P Hegyi, S Ábrahám","doi":"10.1007/s10151-025-03110-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The mesentery might be involved in the pathogenesis of Crohn's disease (CD). As a result of scarce and conflicting data, it is debatable whether removal during intestinal resections could influence postsurgical outcome. We aimed to investigate the association between the extent of mesenteric excision during intestinal resections and postoperative complications and recurrence.</p><p><strong>Methods: </strong>We conducted a systematic search in five databases on 29 July 2024 for studies reporting outcomes in patients with CD who underwent intestinal resections with extended mesenteric excision (EME) compared with limited mesenteric excision (LME). Pooled odds ratios (ORs) with 95% confidence intervals (CI) were calculated using the random-effects model. We assessed the risk of bias using the ROBINS-I and RoB2 tool and evaluated the certainty of evidence according to the GRADE Working Group recommendations.</p><p><strong>Results: </strong>We retrieved data from six studies, covering 4590 patients. The pooled data showed no significant difference between EME and LME patients regarding surgical recurrence (OR 0.3; 95% CI 0.02-3.73; p = 0.176), overall postoperative complications (OR 0.78; 95% CI 0.33-1.82, p = 0.329), anastomotic leak (OR 0.76, 95% CI 0.09-6.85, p = 0.722), surgical site infection (OR 0.84, 95% CI 0.3-2.36, p = 0.539), reoperation rate (OR 1.09, 95% CI 0.33-3.58, p = 0.783), or hospitalization (MD - 0.33 (95% CI - 1.8 to 1.15, p = 0.53). Individual studies reported similar results regarding 6 months follow-up endoscopic recurrence. The certainty of evidence was very low and low, respectively.</p><p><strong>Conclusion: </strong>Extended mesenteric excision is not statistically associated with improved postoperative complications or postoperative recurrence. Results should be interpreted cautiously because of the small number of studies; hence, randomized, long-term, controlled trials are needed.</p>","PeriodicalId":51192,"journal":{"name":"Techniques in Coloproctology","volume":"29 1","pages":"79"},"PeriodicalIF":2.9000,"publicationDate":"2025-03-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11890256/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Techniques in Coloproctology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s10151-025-03110-w","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The mesentery might be involved in the pathogenesis of Crohn's disease (CD). As a result of scarce and conflicting data, it is debatable whether removal during intestinal resections could influence postsurgical outcome. We aimed to investigate the association between the extent of mesenteric excision during intestinal resections and postoperative complications and recurrence.
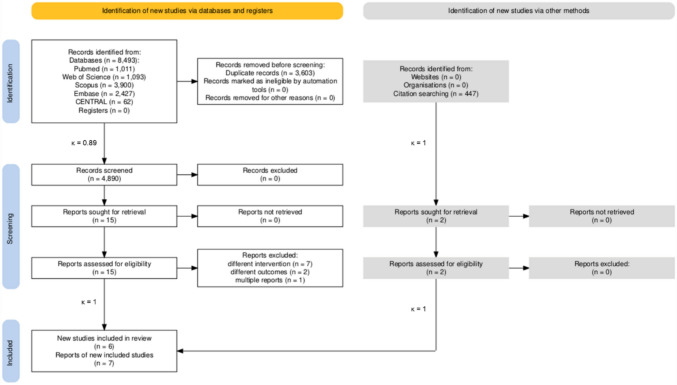
Methods: We conducted a systematic search in five databases on 29 July 2024 for studies reporting outcomes in patients with CD who underwent intestinal resections with extended mesenteric excision (EME) compared with limited mesenteric excision (LME). Pooled odds ratios (ORs) with 95% confidence intervals (CI) were calculated using the random-effects model. We assessed the risk of bias using the ROBINS-I and RoB2 tool and evaluated the certainty of evidence according to the GRADE Working Group recommendations.
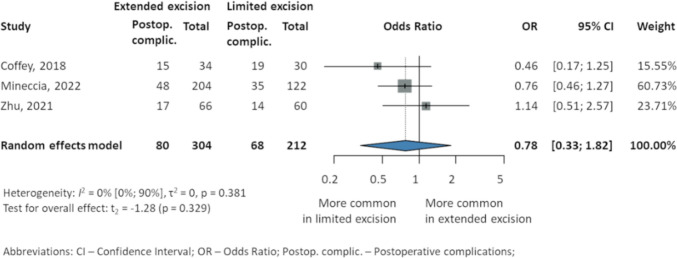
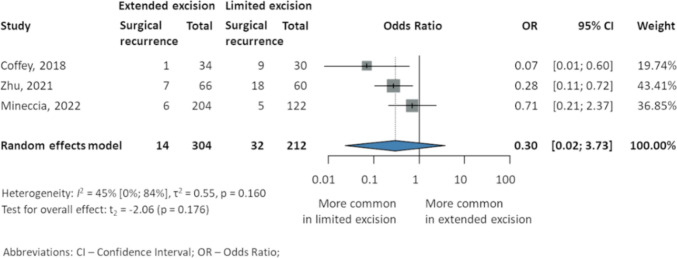
Results: We retrieved data from six studies, covering 4590 patients. The pooled data showed no significant difference between EME and LME patients regarding surgical recurrence (OR 0.3; 95% CI 0.02-3.73; p = 0.176), overall postoperative complications (OR 0.78; 95% CI 0.33-1.82, p = 0.329), anastomotic leak (OR 0.76, 95% CI 0.09-6.85, p = 0.722), surgical site infection (OR 0.84, 95% CI 0.3-2.36, p = 0.539), reoperation rate (OR 1.09, 95% CI 0.33-3.58, p = 0.783), or hospitalization (MD - 0.33 (95% CI - 1.8 to 1.15, p = 0.53). Individual studies reported similar results regarding 6 months follow-up endoscopic recurrence. The certainty of evidence was very low and low, respectively.
Conclusion: Extended mesenteric excision is not statistically associated with improved postoperative complications or postoperative recurrence. Results should be interpreted cautiously because of the small number of studies; hence, randomized, long-term, controlled trials are needed.
背景:肠系膜可能参与克罗恩病(CD)的发病机制。由于缺乏和相互矛盾的数据,肠切除术期间切除是否会影响术后结果是有争议的。我们的目的是研究肠切除术中肠系膜切除的范围与术后并发症和复发之间的关系。方法:我们于2024年7月29日在5个数据库中进行了系统检索,以报告CD患者接受肠切除术合并扩展肠系膜切除术(EME)与有限肠系膜切除术(LME)的结果。采用随机效应模型计算合并优势比(ORs)和95%置信区间(CI)。我们使用ROBINS-I和RoB2工具评估偏倚风险,并根据GRADE工作组的建议评估证据的确定性。结果:我们从6项研究中检索数据,涵盖4590例患者。汇总数据显示,EME和LME患者在手术复发方面无显著差异(OR 0.3;95% ci 0.02-3.73;p = 0.176),总体术后并发症(OR 0.78;95% CI 0.33-1.82, p = 0.329)、吻合口漏(OR 0.76, 95% CI 0.09-6.85, p = 0.722)、手术部位感染(OR 0.84, 95% CI 0.3-2.36, p = 0.539)、再手术率(OR 1.09, 95% CI 0.33-3.58, p = 0.783)、住院率(MD - 0.33 (95% CI -1.8 - 1.15, p = 0.53)。个别研究报告了随访6个月的内镜下复发的类似结果。证据的确定性分别非常低和低。结论:扩大肠系膜切除术与术后并发症的改善或术后复发无统计学相关性。由于研究数量少,结果应谨慎解释;因此,需要随机、长期、对照试验。
期刊介绍:
Techniques in Coloproctology is an international journal fully devoted to diagnostic and operative procedures carried out in the management of colorectal diseases. Imaging, clinical physiology, laparoscopy, open abdominal surgery and proctoperineology are the main topics covered by the journal. Reviews, original articles, technical notes and short communications with many detailed illustrations render this publication indispensable for coloproctologists and related specialists. Both surgeons and gastroenterologists are represented on the distinguished Editorial Board, together with pathologists, radiologists and basic scientists from all over the world. The journal is strongly recommended to those who wish to be updated on recent developments in the field, and improve the standards of their work.
Manuscripts submitted for publication must contain a statement to the effect that all human studies have been reviewed by the appropriate ethics committee and have therefore been performed in accordance with the ethical standards laid down in an appropriate version of the 1965 Declaration of Helsinki. It should also be stated clearly in the text that all persons gave their informed consent prior to their inclusion in the study. Details that might disclose the identity of the subjects under study should be omitted. Reports of animal experiments must state that the Principles of Laboratory Animal Care (NIH publication no. 86-23 revised 1985) were followed as were applicable national laws (e.g. the current version of the German Law on the Protection of Animals). The Editor-in-Chief reserves the right to reject manuscripts that do not comply with the above-mentioned requirements. Authors will be held responsible for false statements or for failure to fulfill such requirements.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
