Siying S Li, Kimberlyn McGrail, Rhonda J Rosychuk, Michael R Law, Corinne M Hohl
{"title":"Outcomes for people experiencing homelessness with COVID-19 presenting to emergency departments in Canada, compared with housed patients.","authors":"Siying S Li, Kimberlyn McGrail, Rhonda J Rosychuk, Michael R Law, Corinne M Hohl","doi":"10.1503/cmaj.241282","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Whether people experiencing homelessness (PEH) have different COVID-19 outcomes than housed patients in Canada remains unclear. We sought to ascertain whether rates of in-hospital mortality, hospital admission, critical care admission, and mechanical ventilation differed between PEH and housed people with symptomatic SARS-CoV-2 infection.</p><p><strong>Methods: </strong>We conducted a propensity score-matched cohort study to compare the outcomes of PEH and housed patients presenting to emergency departments for acute symptomatic COVID-19. We used data from the Canadian COVID-19 Emergency Department Rapid Response Network (CCEDRRN) registry. Covariates in our propensity score model included age, sex, comorbidities, substance use, vaccination status, previous do-not-resuscitate documentation, hospital type, province and calendar quarter of presentation to the emergency department, symptom duration, and severity of illness on presentation.</p><p><strong>Results: </strong>We found no difference in mortality for PEH (3%) compared with a propensity score-matched cohort of housed patients (3%) (odds ratio [OR] 0.87, 95% confidence interval [CI] 0.43-1.74). We also found no difference in admission rates for PEH (44%) versus housed patients (45%). There was a reduced rate of critical care admission for PEH compared with housed patients (OR 0.66, 95% CI 0.44-1.00), and a trend toward decreased use of mechanical ventilation for PEH versus housed patients, which was not significant (OR 0.60, 95% CI 0.35-1.02).</p><p><strong>Interpretation: </strong>We found no difference in mortality for PEH with COVID-19 compared with those who were housed. A signal for reduced critical care admission among PEH may reflect differential treatment unrelated to clinical characteristics that we matched for. Future research on resource allocation during pandemics could shed light on potential inequities for vulnerable populations and how best to address them.</p>","PeriodicalId":9609,"journal":{"name":"Canadian Medical Association journal","volume":"197 9","pages":"E236-E243"},"PeriodicalIF":11.3000,"publicationDate":"2025-03-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11908794/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Medical Association journal","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1503/cmaj.241282","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Whether people experiencing homelessness (PEH) have different COVID-19 outcomes than housed patients in Canada remains unclear. We sought to ascertain whether rates of in-hospital mortality, hospital admission, critical care admission, and mechanical ventilation differed between PEH and housed people with symptomatic SARS-CoV-2 infection.
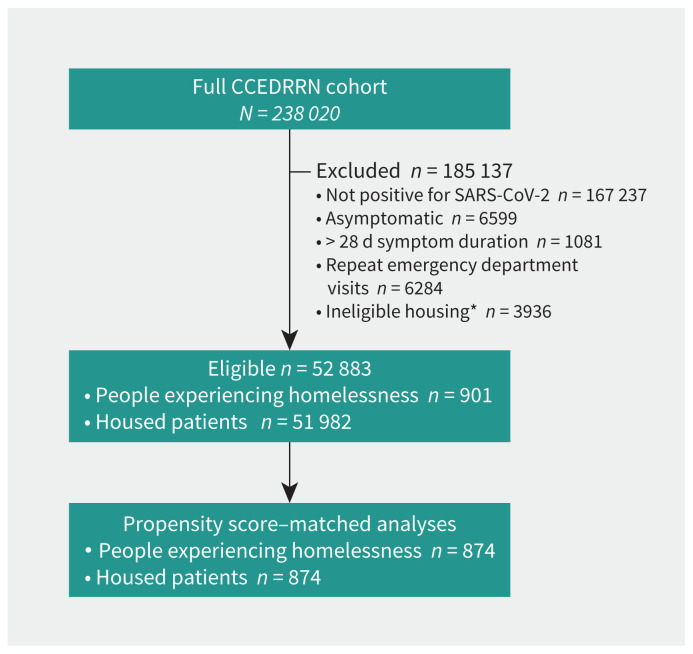
Methods: We conducted a propensity score-matched cohort study to compare the outcomes of PEH and housed patients presenting to emergency departments for acute symptomatic COVID-19. We used data from the Canadian COVID-19 Emergency Department Rapid Response Network (CCEDRRN) registry. Covariates in our propensity score model included age, sex, comorbidities, substance use, vaccination status, previous do-not-resuscitate documentation, hospital type, province and calendar quarter of presentation to the emergency department, symptom duration, and severity of illness on presentation.
Results: We found no difference in mortality for PEH (3%) compared with a propensity score-matched cohort of housed patients (3%) (odds ratio [OR] 0.87, 95% confidence interval [CI] 0.43-1.74). We also found no difference in admission rates for PEH (44%) versus housed patients (45%). There was a reduced rate of critical care admission for PEH compared with housed patients (OR 0.66, 95% CI 0.44-1.00), and a trend toward decreased use of mechanical ventilation for PEH versus housed patients, which was not significant (OR 0.60, 95% CI 0.35-1.02).
Interpretation: We found no difference in mortality for PEH with COVID-19 compared with those who were housed. A signal for reduced critical care admission among PEH may reflect differential treatment unrelated to clinical characteristics that we matched for. Future research on resource allocation during pandemics could shed light on potential inequities for vulnerable populations and how best to address them.
期刊介绍:
CMAJ (Canadian Medical Association Journal) is a peer-reviewed general medical journal renowned for publishing original research, commentaries, analyses, reviews, clinical practice updates, and editorials. Led by Editor-in-Chief Dr. Kirsten Patrick, it has a significant impact on healthcare in Canada and globally, with a 2022 impact factor of 17.4.
Its mission is to promote knowledge vital for the health of Canadians and the global community, guided by values of service, evidence, and integrity. The journal's vision emphasizes the importance of the best evidence, practice, and health outcomes.
CMAJ covers a broad range of topics, focusing on contributing to the evidence base, influencing clinical practice, and raising awareness of pressing health issues among policymakers and the public. Since 2020, with the appointment of a Lead of Patient Involvement, CMAJ is committed to integrating patients into its governance and operations, encouraging their content submissions.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
