Management of high-surgical-risk patients with acute cholecystitis following percutaneous cholecystostomy: results of an international Delphi consensus study.
Antonio Pesce, Camilo Ramírez-Giraldo, Nikolaos-Achilleas Arkoudis, George Ramsay, Georgi Popivanov, Kurinchi Gurusamy, Natalia Bejarano, Maria Irene Bellini, Massimiliano Allegritti, Jacopo Tesei, Alessandro Gemini, Augusto Lauro, Matteo Matteucci, Antonio La Greca, Valerio Cozza, Federico Coccolini, Marco Cannistra', Carlo Boselli, Piero Covarelli, Gianluca Costa, Paolo Bruzzone, Giovanni Domenico Tebala, Simona Meneghini, Vito D'Andrea, Andrea Mingoli, Eugenio Cucinotta, Antonia Rizzuto, Mauro Zago, Paolo Prosperi, Massimo Buononato, Gioia Brachini, Roberto Cirocchi
{"title":"Management of high-surgical-risk patients with acute cholecystitis following percutaneous cholecystostomy: results of an international Delphi consensus study.","authors":"Antonio Pesce, Camilo Ramírez-Giraldo, Nikolaos-Achilleas Arkoudis, George Ramsay, Georgi Popivanov, Kurinchi Gurusamy, Natalia Bejarano, Maria Irene Bellini, Massimiliano Allegritti, Jacopo Tesei, Alessandro Gemini, Augusto Lauro, Matteo Matteucci, Antonio La Greca, Valerio Cozza, Federico Coccolini, Marco Cannistra', Carlo Boselli, Piero Covarelli, Gianluca Costa, Paolo Bruzzone, Giovanni Domenico Tebala, Simona Meneghini, Vito D'Andrea, Andrea Mingoli, Eugenio Cucinotta, Antonia Rizzuto, Mauro Zago, Paolo Prosperi, Massimo Buononato, Gioia Brachini, Roberto Cirocchi","doi":"10.1097/JS9.0000000000002325","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The management of high-surgical-risk patients with moderate to severe acute cholecystitis is challenging in clinical practice. Early laparoscopic cholecystectomy is considered the gold standard for patients who do not respond to conservative treatment. However, for those unfit for surgery due to high risk, alternative treatment options, such as percutaneous cholecystostomy (PC), are available. There are no clear guidelines regarding the management of patients following PC. The primary aim of this study was to propose indications for PC in high-surgical-risk patients with acute cholecystitis and to establish management strategies for gallbladder drainage, either as a bridge to surgery or as a definitive treatment, according to available literature.</p><p><strong>Materials and methods: </strong>After a targeted literature review, International and Italian experts in the field from the Italian Society of Research in Surgery (SIRC) and the Italian Society of Emergency Surgery and Trauma (SICUT) were consulted to provide their evidence-based opinions on the topic. Statements were proposed during subsequent rounds using the Delphi methodology. Ten statements were provided, and the final agreement is presented in this study.</p><p><strong>Results: </strong>Patients with moderate acute cholecystitis, a Charlson Comorbidity Index (CCI) ≥ 6, and American Society of Anesthesiologists-Performance Status (ASA-PS) ≥ 3 who fail conservative treatment should undergo laparoscopic cholecystectomy as the first-line approach. For those with severe acute cholecystitis at high-surgical risk, percutaneous cholecystostomy is recommended to relieve symptoms within 24-48 hours. Once the infection is controlled, we should assess which patients may be candidates for interval laparoscopic cholecystectomy. For patients selected for surgery, laparoscopic cholecystectomy is recommended at least six weeks after PC placement. In patients not suitable for surgery, such as those with CCI ≥ 6 and ASA-PS ≥ 4, percutaneous cholecystostomy should remain in place for at least three weeks, after which, following radiographic confirmation of biliary tree patency, the tube may be removed.</p><p><strong>Conclusions: </strong>This consensus, developed through a multidisciplinary collaboration of interventional radiologists, gastroenterologists, and surgeons, provides a clear and practical guide for managing high-risk surgical patients with acute cholecystitis.</p>","PeriodicalId":14401,"journal":{"name":"International journal of surgery","volume":" ","pages":"3185-3192"},"PeriodicalIF":10.1000,"publicationDate":"2025-05-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12165509/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"International journal of surgery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1097/JS9.0000000000002325","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"SURGERY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: The management of high-surgical-risk patients with moderate to severe acute cholecystitis is challenging in clinical practice. Early laparoscopic cholecystectomy is considered the gold standard for patients who do not respond to conservative treatment. However, for those unfit for surgery due to high risk, alternative treatment options, such as percutaneous cholecystostomy (PC), are available. There are no clear guidelines regarding the management of patients following PC. The primary aim of this study was to propose indications for PC in high-surgical-risk patients with acute cholecystitis and to establish management strategies for gallbladder drainage, either as a bridge to surgery or as a definitive treatment, according to available literature.
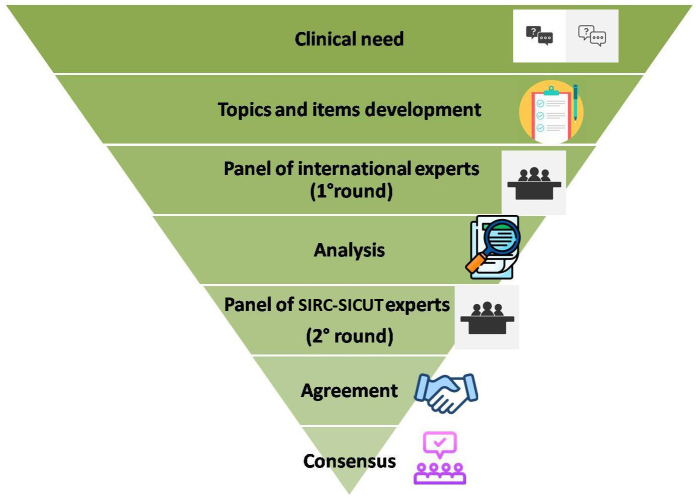
Materials and methods: After a targeted literature review, International and Italian experts in the field from the Italian Society of Research in Surgery (SIRC) and the Italian Society of Emergency Surgery and Trauma (SICUT) were consulted to provide their evidence-based opinions on the topic. Statements were proposed during subsequent rounds using the Delphi methodology. Ten statements were provided, and the final agreement is presented in this study.
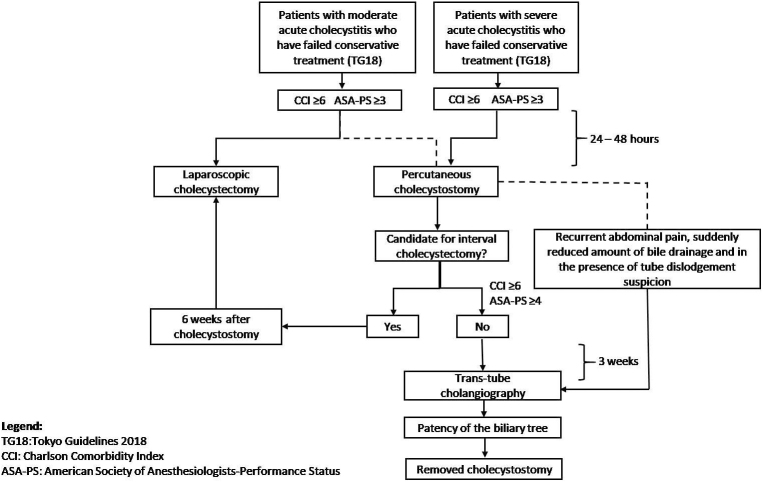
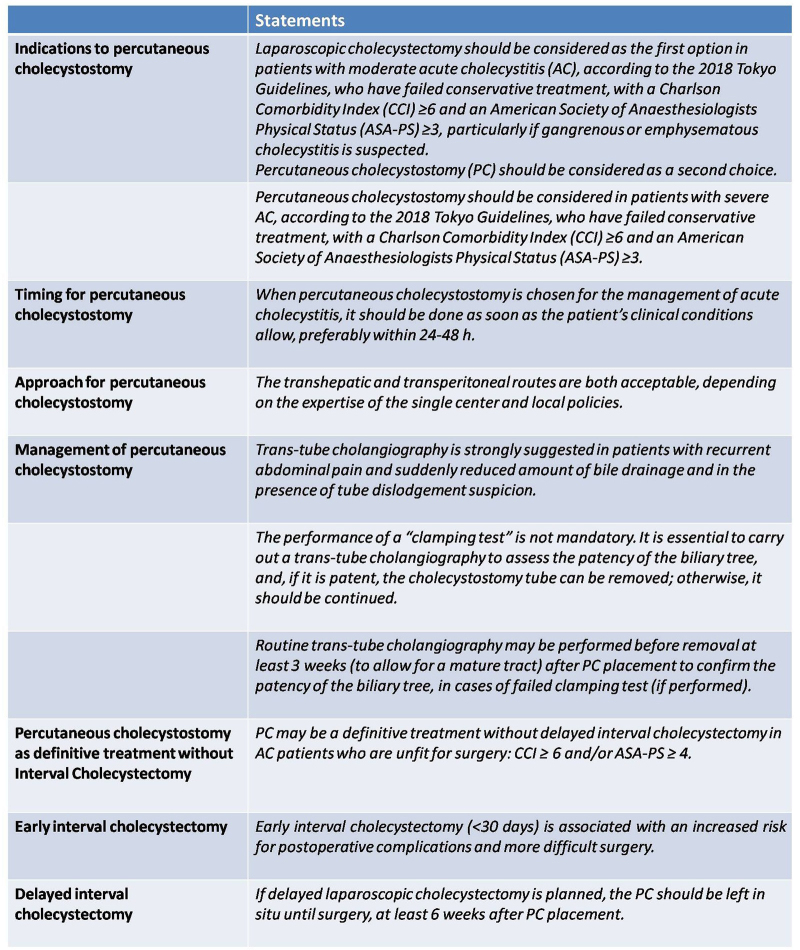
Results: Patients with moderate acute cholecystitis, a Charlson Comorbidity Index (CCI) ≥ 6, and American Society of Anesthesiologists-Performance Status (ASA-PS) ≥ 3 who fail conservative treatment should undergo laparoscopic cholecystectomy as the first-line approach. For those with severe acute cholecystitis at high-surgical risk, percutaneous cholecystostomy is recommended to relieve symptoms within 24-48 hours. Once the infection is controlled, we should assess which patients may be candidates for interval laparoscopic cholecystectomy. For patients selected for surgery, laparoscopic cholecystectomy is recommended at least six weeks after PC placement. In patients not suitable for surgery, such as those with CCI ≥ 6 and ASA-PS ≥ 4, percutaneous cholecystostomy should remain in place for at least three weeks, after which, following radiographic confirmation of biliary tree patency, the tube may be removed.
Conclusions: This consensus, developed through a multidisciplinary collaboration of interventional radiologists, gastroenterologists, and surgeons, provides a clear and practical guide for managing high-risk surgical patients with acute cholecystitis.
期刊介绍:
The International Journal of Surgery (IJS) has a broad scope, encompassing all surgical specialties. Its primary objective is to facilitate the exchange of crucial ideas and lines of thought between and across these specialties.By doing so, the journal aims to counter the growing trend of increasing sub-specialization, which can result in "tunnel-vision" and the isolation of significant surgical advancements within specific specialties.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
