{"title":"A complicated Vogt-Koyanagi-Harada presenting with bilateral papillitis in a 5-year-old- case report.","authors":"Salem Almerri, Raed Behbehani","doi":"10.1186/s12348-025-00481-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>We report a case of a 5-year-old patient with Vogt-Koyanagi-Harada presenting atypically with bilateral papillitis and refractory inflammation, leading to uveitic glaucoma and necessitating an escalation of adalimumab to 40 mg biweekly.</p><p><strong>Observations: </strong>A 5-year-old girl presented with a 3-week history of eye redness, excessive lacrimation, and photophobia. Her medical history was unremarkable. On examination, her best-corrected visual acuity (BCVA) were 20/80 and 20/100 in right and left eye, respectively, with normal intraocular pressure (IOP). Anterior segment examination revealed fine keratic precipitates, anterior chamber inflammation (+ 4 cells and flare), and semi-dilated pupils with posterior synechiae. Posterior segment evaluation was limited by severe vitritis. Laboratory investigations were unremarkable except for HLA-DR4, DR52, and DR53 positivity. Optical coherence tomography (OCT) of the optic nerve showed increased retinal nerve thickness. Initial treatment with corticosteroids and methotrexate failed to achieve remission. Attempts to taper corticosteroids resulted in recurrence of anterior chamber flare, prompting the introduction of adalimumab at 20 mg/biweekly. Despite relative stability, persistent anterior chamber inflammation and subsequent corticosteroid tapering led to the development of uncontrolled uveitic glaucoma requiring surgical peripheral iridectomy. Postoperatively, adalimumab was escalated to 40 mg/biweekly, enabling successful tapering of corticosteroids. Over a 9-month follow-up period, the patient remained flare-free, with BCVA improving to 20/20 in both eyes.</p><p><strong>Conclusions and importance: </strong>This case highlights an atypical presentation of VKH in a preschool-aged child, characterized by bilateral papillitis without exudative retinal detachment. Escalation of adalimumab to 40 mg biweekly effectively controlled inflammation, facilitated corticosteroid tapering, and preserved visual acuity.</p>","PeriodicalId":16600,"journal":{"name":"Journal of Ophthalmic Inflammation and Infection","volume":"15 1","pages":"27"},"PeriodicalIF":2.3000,"publicationDate":"2025-03-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11909293/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Ophthalmic Inflammation and Infection","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s12348-025-00481-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"OPHTHALMOLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Purpose: We report a case of a 5-year-old patient with Vogt-Koyanagi-Harada presenting atypically with bilateral papillitis and refractory inflammation, leading to uveitic glaucoma and necessitating an escalation of adalimumab to 40 mg biweekly.
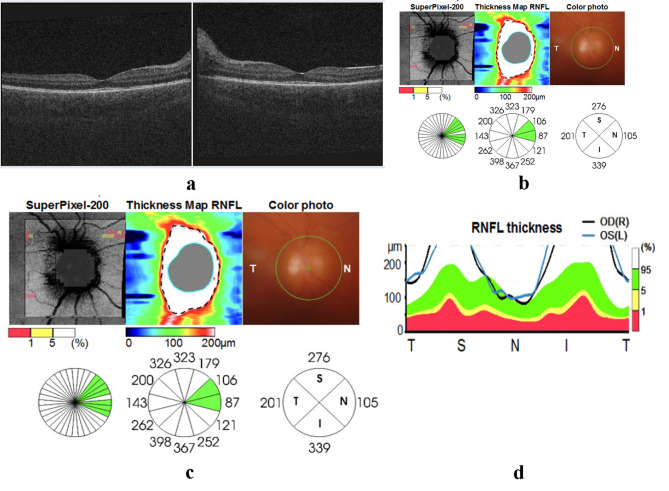
Observations: A 5-year-old girl presented with a 3-week history of eye redness, excessive lacrimation, and photophobia. Her medical history was unremarkable. On examination, her best-corrected visual acuity (BCVA) were 20/80 and 20/100 in right and left eye, respectively, with normal intraocular pressure (IOP). Anterior segment examination revealed fine keratic precipitates, anterior chamber inflammation (+ 4 cells and flare), and semi-dilated pupils with posterior synechiae. Posterior segment evaluation was limited by severe vitritis. Laboratory investigations were unremarkable except for HLA-DR4, DR52, and DR53 positivity. Optical coherence tomography (OCT) of the optic nerve showed increased retinal nerve thickness. Initial treatment with corticosteroids and methotrexate failed to achieve remission. Attempts to taper corticosteroids resulted in recurrence of anterior chamber flare, prompting the introduction of adalimumab at 20 mg/biweekly. Despite relative stability, persistent anterior chamber inflammation and subsequent corticosteroid tapering led to the development of uncontrolled uveitic glaucoma requiring surgical peripheral iridectomy. Postoperatively, adalimumab was escalated to 40 mg/biweekly, enabling successful tapering of corticosteroids. Over a 9-month follow-up period, the patient remained flare-free, with BCVA improving to 20/20 in both eyes.
Conclusions and importance: This case highlights an atypical presentation of VKH in a preschool-aged child, characterized by bilateral papillitis without exudative retinal detachment. Escalation of adalimumab to 40 mg biweekly effectively controlled inflammation, facilitated corticosteroid tapering, and preserved visual acuity.



 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
