{"title":"Diagnostic process, misdiagnosis and bias in suspected idiopathic intracranial hypertension: a retrospective observational cohort study.","authors":"Nadja Skadkær Hansen, Johanne Juhl Korsbæk, Steffen Hamann, Rigmor Højland Jensen","doi":"10.1136/bmjno-2024-000863","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Misdiagnosis of idiopathic intracranial hypertension (IIH) is prevalent and potentially harmful. We evaluated the diagnostic process of IIH and the impact of implementing a National Guideline (NG) on IIH management to improve patient care.</p><p><strong>Method: </strong>In this observational retrospective study, we retrieved data on diagnostic investigations, duration, errors and causes for suspecting IIH from patients referred to the Danish Headache Center by suspected new-onset IIH from January 2020 to September 2022. We compared outcomes by final diagnosis (true vs disproven IIH) and the period before and after implementation of the NG. Level of significance was Bonferroni adjusted to p<0.002.</p><p><strong>Results: </strong>96 patients were referred. We confirmed IIH in 27 (28%) and disproved IIH in 69 (72%) whose final diagnoses were predominantly headache disorders (70%) and pseudo-papilloedema (12%). True IIH was discovered by optic disc oedema (n=25, none detected by neurologists); neuroimaging indicating elevated intracranial pressure (n=1) or a typical clinical phenotype (n=1) aided little but often elicited IIH suspicion suggesting anchoring bias with premature closure. Misdiagnosis affected 11% (n=11). Diagnostic workup was more comprehensive and faster in true IIH (p<0.001). Mismanagement dropped by implementation of the NG (from 44% to 20%, p=0.02).</p><p><strong>Conclusion: </strong>Optic disc oedema is the most predictive determinant of true IIH; neuroimaging and phenotype alone have poor diagnostic value and introduce bias. Fundus exam is urgent and decisive in suspected IIH and should guide diagnostic strategy to mitigate unnecessary investigations and preserve vision. An NG reduced diagnostic errors and optimised the diagnostic process.</p>","PeriodicalId":52754,"journal":{"name":"BMJ Neurology Open","volume":"7 1","pages":"e000863"},"PeriodicalIF":2.4000,"publicationDate":"2025-03-12","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11911662/pdf/","citationCount":"0","resultStr":null,"platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMJ Neurology Open","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1136/bmjno-2024-000863","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2025/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
Abstract
Background: Misdiagnosis of idiopathic intracranial hypertension (IIH) is prevalent and potentially harmful. We evaluated the diagnostic process of IIH and the impact of implementing a National Guideline (NG) on IIH management to improve patient care.
Method: In this observational retrospective study, we retrieved data on diagnostic investigations, duration, errors and causes for suspecting IIH from patients referred to the Danish Headache Center by suspected new-onset IIH from January 2020 to September 2022. We compared outcomes by final diagnosis (true vs disproven IIH) and the period before and after implementation of the NG. Level of significance was Bonferroni adjusted to p<0.002.
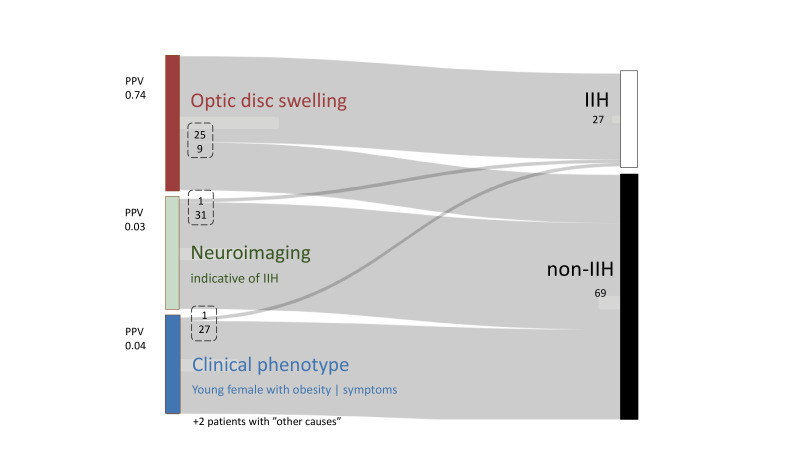
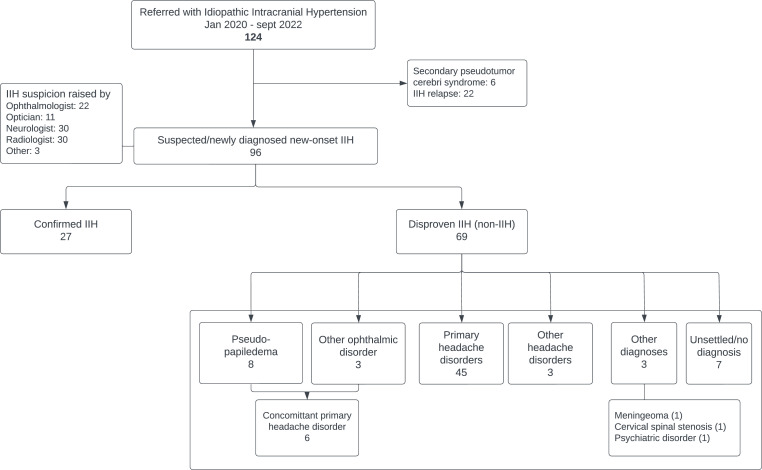
Results: 96 patients were referred. We confirmed IIH in 27 (28%) and disproved IIH in 69 (72%) whose final diagnoses were predominantly headache disorders (70%) and pseudo-papilloedema (12%). True IIH was discovered by optic disc oedema (n=25, none detected by neurologists); neuroimaging indicating elevated intracranial pressure (n=1) or a typical clinical phenotype (n=1) aided little but often elicited IIH suspicion suggesting anchoring bias with premature closure. Misdiagnosis affected 11% (n=11). Diagnostic workup was more comprehensive and faster in true IIH (p<0.001). Mismanagement dropped by implementation of the NG (from 44% to 20%, p=0.02).
Conclusion: Optic disc oedema is the most predictive determinant of true IIH; neuroimaging and phenotype alone have poor diagnostic value and introduce bias. Fundus exam is urgent and decisive in suspected IIH and should guide diagnostic strategy to mitigate unnecessary investigations and preserve vision. An NG reduced diagnostic errors and optimised the diagnostic process.




 分享
分享
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式: 扫码关注我们
扫码关注我们
